Abstract
Melanocytoma is a rare benign lesion arising from leptomeningeal melanocytes. Meningeal melanocytomas are commonly seen in the thoracic region of the spinal canal and may also arise in the cervical or lumbar region, most often located in the intradural extramedullary compartment 1. To our knowledge, only 21 cases of intramedullary melanocytomas have been reported in the literature to date. The authors present a rare case of thoracic intramedullary melanocytoma and the review of the literature pointing out the role of diagnosis, surgical treatment and follow-up.
Author Contributions
Academic Editor: Pranshu Mohindra, Department of Human Oncology, UW-Madison School of Medicine and Public Health.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2014 Ruggeri AG, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Melanocytoma is a rare benign lesion arising from leptomeningeal melanocytes. It was first described by Limas and Tio in 1972. Melanocytoma usually has an intracranial localization but may occur in the spine too. Meningeal melanocytomas are commonly seen in the thoracic region of the spinal canal and may also arise in the cervical or lumbar region, most often located in the intradural extramedullary compartment 1. To our knowledge, only 21 cases of intramedullary melanocytomas have been reported in the literature to date. The authors present a rare case of thoracic intramedullary melanocytoma and the review of the literature.
Case Description
A 74-year-old woman presented complaining a several-month history of increasing thoracic back pain and left leg pain. Neurological examination demonstrated a spastic paraparetic gait and hyperreflexia of the lower limbs. Spinal magnetic resonance imaging revealed an intramedullary mass extending from T7 to T11 measuring 22 x 12 x 15 mm, slightly hyperintense on T1weighted images and hypointense on T2 weighted sequences and showed mild and heterogeneous enhancement after injection of gadolinium (Figure 1). Motor and somatosensory evoked potentials (SSEP) were recorded during surgery. A T7-T11 laminectomy and posterior midline myelotomy was performed. The exposed black and rigid tissue was removed en block (Figure 2). Gross total removal was achieved, as confirmed by MRI with and without contrast 24 hours after operation.
Figure 1.Spinal magnetic resonance imaging showing an intramedullary mass extending from T7-11 A) hypointense on T2 weighted sequences and B) slightly hyperintense on T1weighted imagines with mild and heterogeneous enhancement after the injection of gadolinium.
Figure 2.A) Intraoperative picture. B) Photomicrograph of the bleached tumor cells displaying immuno-positivity for HMB-45.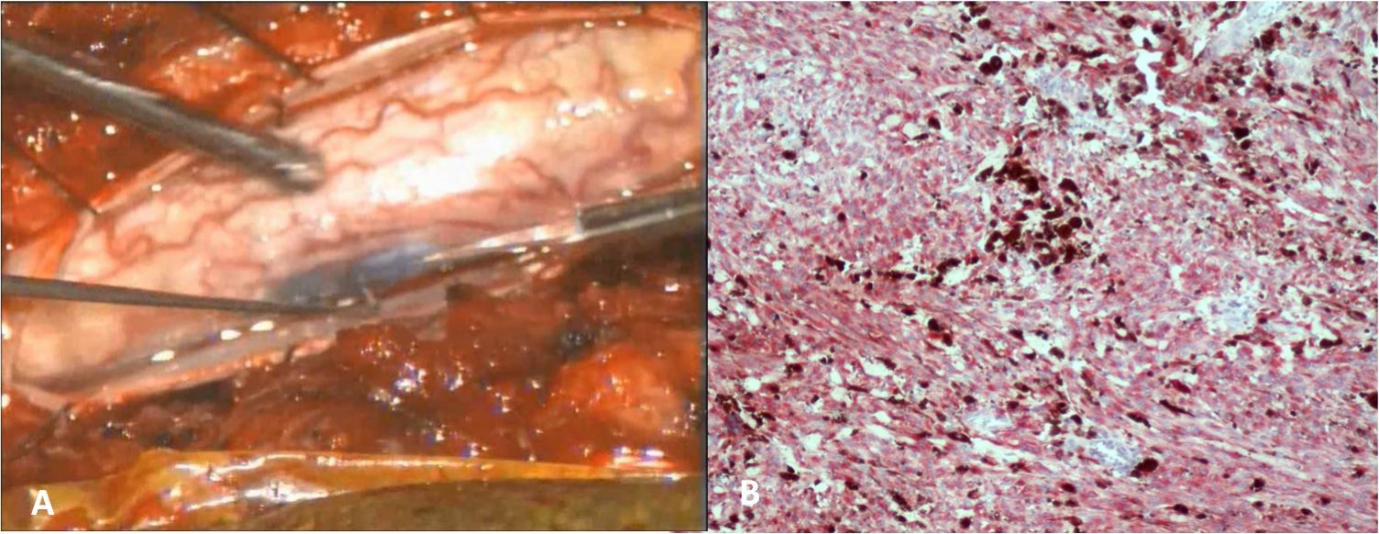
The patient had no bowel or bladder dysfunction but preexisting left hemiparesis worsened immediately after surgery. She underwent rehabilitation, and at 2 months post surgery had regained full strength. Histological examination revealed neoplasia mainly consisting of spindle-shaped monomorphic cells with clearly visible nucleoli and melanin-rich cytoplasm. It exhibits low mitotic activity, and stains positively with HMB-45 and S-100, indicating cells of melanocytic origin. The histological diagnosis was consistent with a melanocytoma.
Review of the Literature
A computer-aided search of MEDLINE was conducted from 1990 to 2012. The search was performed using keywords as “melanocytoma”, “intramedullary spinal cord tumor” and was limited to human studies.
Only 21 cases have been described in literature to date, we summarize in the Table 110 of those cases.
Table 1. Summary of intramedullary Melanocytomas| Authors & year | Age | Sex | Location | Resection | Follow-up | Local | Metastasis | Radio therapy |
| of lesion | period | relapse | ||||||
| Barth et al. 1993 4 | 49 | F | T10-T12 | 2 subtotal | 4 years | Yes | Yes | No |
| Glick et al. 1997 2 | 69 | M | C1-C2 | Total | 5 years | No | No | No |
| Glick et al. 1997 3 | 39 | F | T8-T9 | Subtotal | 1 year | No | No | Yes |
| after surgery | ||||||||
| Delhaye et al. 2001 | 38 | F | T6-T9 | 2 subtotal | 4 years | Yes | Yes | No |
| Turhan et al. 2004 9 | 19 | F | T8 | Total | 3 years | No | No | No |
| Van Paesschen et al. 2004 | 51 | M | C1-C2 | Total | - | No | No | No |
| Horn et al. 2008 | 37 | F | C1-3 | Total | 3 years | Yes | No | No |
| Caruso et al. 2009 | 62 | M | T11 | Total | 2 years | No | No | No |
| Karikari IO et al. 2009 | 32 | F | T10 | Total | 3 months | No | No | No |
| Eskandari R, et al 2010 5 | 45 | M | T11 | Subtotal | 3 years | No | yes | Yes |
| M. Muthappan et al 2011 10 | 61 | F | C3-4 | Total | 3 years | No | No | No |
As we observed in the literature this tumor is most commonly found in women with an average age of 45,9 years (range, 19–79 years). The biological behavior is most commonly benign, although these tumours are slow growing, they have a propensity to recur, metastasize via the cerebrospinal fluid, and undergo malignant transformation. In the literature 12 cases out of 21 have been radically removed and never relapsed (follow up 3,5 years). 2, 3, 4 Tumour recurrence has been reported as early as three months after surgical resection; hence, it is crucial that these patients are followed up regularly with serial MRI and clinical assessment to identify early recurrence. In the event of local recurrence, operative resection is a reasonable treatment option, although it may be associated with significant morbidity; the alternative is radiation treatment. In the literature is reported only 1 case of local relapse treated with radiotherapy, in the other cases close follow-up monitoring was undertaken.
The goal of treatment should be complete/gross total resection with preservation of neurological function. Radiotherapy is generally provided when resection is incomplete 2, 3. In the literature 5 cases of subtotal removal have been described. In 3 of the 5 cases in which tumor removal was subtotal, local recurrence occurred; and in 4 cases there was metastatic spread via the CSF of these 2 patients underwent 2 partial removals. The only case of subtotal removal without subsequent recurrence was the only case in which radiotherapy 2, 3 was performed.
Discussion
Melanocytomas are neural crest-derived cells which are normally found within the basal layer of the epidermis and the leptomeninges that cover the base of brain and the brain stem. Moreover, the highest concentration of melanocytes is seen ventrolateral to the medulla oblongata and upper cervical levels of spinal leptomeniges. The term ‘meningeal melanocytoma’ was first proposed by Limas and Tio in 1972 based on ultrastructural features to differentiate these benign pigmented tumors from those originating from meningothelial fibroblasts. Since then, less than 100 cases have been reported in the literature. Macroscopically, melanocytoma can be dark-to-tan (Figure 3), and is commonly composed, microscopically, of nests of spindle-shaped cells with small nucleoli and eosinophilic cytoplasm. The World Health Organization has classified primary melanocytic tumors of the nervous system into diffuse melanocytosis, melanocytoma, malignant melanoma and meningeal melanomatosis . All melanin-containing tumors show presence of spindle or epithelioid cells arranged in sheets, bundles, nests or whorls. The difference between melanocytoma and melanoma is the low mitotic activity and the absence of nuclear atypia, as shown by low reactivity with Ki-67. Moreover a positive immunoreactivity for S100 protein, Vimentin, HMB- 45 favors the diagnosis of a melanocytic tumor. Malignant transformation of a melanocytoma to melanoma following complete excision has been reported in the literature. This is why the goal of the treatment should be gross total resection with preservation of neurological function. These lesions are exceedingly rare. Approximately 50% of the cases are found intracranially, mostly observed in supratentorial locations, and the other half in the spinal canal, mostly in the thoracic region. They are usually intradural and extramedullary, but can be either extradural or intramedullary. Intramedullary melanocytomas are extremely rare. In the review of the literature 16 cases described origin from thoracic region as our case and only 5 cases from cervical spine. Spinal melanocytomas are slowly growing tumors that usually present with symptoms of mass effect, such as pain, myelopathy, spastic paraparetic gait. In rare cases, however, they may have small hemorrhages and present with signs of superficial siderosis. These neoplasms are most commonly found as solitary lesions, but can present as multifocal lesions or can be disseminated along the arachnoid and dura mater.
Figure 3.the black and rigid tissue removed en block
Typical MRI show an intramedullary lesion that appears isointense on T1-weighted sequences, hypointense on T2 weighted sequences, and enhances homogenously with gadolinium. These signal features are inconsistent due to the variable degree of tumour melanisation, which affects the signal characteristics on MRI. Hence, meningeal melanocytoma should be included in the differential diagnosis of lesions as ependymoma, meningioma and intramedullary astrocytoma 5, 6, 7.
Although these tumours are slow growing, they have a propensity to recur, 7 out of 21 cases described in the literature and to metastasize, 4 cases found in the literature, via the cerebrospinal fluid, and undergo malignant transformation. Rades and Schild reported that some patients with a meningeal melanocytoma might have recurrence even after complete tumor resection 8. They proposed then radiotherapy, and recommend postoperative radiotherapy, even in cases of complete resection. However, there are limited long-term clinical data regarding this pathology. The patient we treated didn’t undergo radiotherapy and is now tumor free. The review of the literature shows only 3 cases treated with radiotherapy because of a partial removal of the lesion.
Tumour recurrence has been reported as early as three months after surgical resection; hence, it is crucial that these patients are followed up regularly with serial MRI and clinical assessment to identify early recurrence. In the event of local recurrence, operative resection is a reasonable treatment option, although it may be associated with significant morbidity; the alternative is radiation treatment. Additional information is required regarding the long term outcome of melanocytoma after surgical resection and radiotherapy, to enable improved treatment strategies.
Conclusions
Intramedullary melanocytoma is extremely rare. The majority of these leptomeningeal tumors are extramedullary, and only few cases of intramedullary tumors have been reported. As with most rare tumors, only case reports are available for reference; thus, no gold standard exists for the definitive treatment and follow-up of patients with these tumors. We favor radical tumor resection when possible and close follow up monitoring since these tumors can recur. Radiation therapy should be reserved for those cases in which complete resection is not possible or in which there is recurrence.
References
- 1.Chacko G, Rajshekhar V. (2008) Thoracic intramedullary melanocytoma with long-term follow-up. , J Neurosurg Spine 9, 589-92.
- 2.Glick R, Baker C, Husain S, Hays A, Hibshoosh H. (1997) Primary melanocytomas of the spinal cord: a report of seven cases. , Clin Neuropathol 16, 127-132.
- 4.Barth A, Pizzolato G P, Berney J. (1993) Intramedullary meningeal melanocytoma. , Neurochirurgie 39, 188-194.
- 5.Landi A, V Di Norcia, Dugoni D E. (2010) Intramedullary non-specific inflammatory lesion of thoracic spine: A case report. World journal of surgical oncology. 15, 8-3.
- 6.Landi A, Pietrantonio A, Marotta N, Mancarella C, Delfini R.(Mar22,2013) Intra-Extramedullary Drainage as an Effective Option for Treatment of Intramedullary Ependymal Cyst of Thoracic Spine: Technical Note Journal of Neurological Surgery Part A: Central European Neurosurgery.
- 7.Landi A, Mancarella C, Marotta N. (2013) Diagnosis and Treatment of Paragangliomas of the Filum Terminale, an Extremely Rare Entity: Personal Experience and Literature Review. , J Spine 2, 3-001.
- 8.Ferracini R, Gardini G, Brisigotti M, Lanzanova G, Manetto V et al. (1980) Metastasizing meningeal melanocytoma. , Tumori 66, 405-408.