
Abstract
Background:
Gastric cancer (GC) ranks as the fourth most common cancer and the second leading cause of cancer deaths worldwide. Epstein-Barr virus is a well-known oncogenic virus, it is responsible for 10% of gastric carcinomas across the world. The aim of study was to determine the prevalence of EBV associated with GC in Sudanese patients.
Method:
Fifty Paraffin embedded blocks of gastric biopsy specimens diagnosed as gastric carcinoma were collected from Soba university hospital and Ribat teaching hospital, Khartoum, Sudan. DNA was extracted from the paraffin-embedded tissue, and then Epstein-Barr virus gene was detected by polymerase chain reaction (PCR).
Result:
Among the gastric biopsy specimens 27 (54.0%) were of male and 23(46.0%) were of female. Eleven EBV positive samples were found in gastric carcinomas (22.0%), 8 (72.7%) were of male and 3(27.2%) were of female. The mean age of the patients was 56 years, the most positive cases were between 50-59 years old, and (10%) of them are alive in Khartoum.
Conclusions:
There exists an association between EBV and gastric carcinoma in some Sudanese patients.
Author Contributions
Academic Editor: Charlic Gourley, University of Edinburgh Cancer Research UK Centre
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Ibtihal omer, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Cancer is the one of leading cause of death in developed and developing countries 1. In 2012 about 14 million new cases and 8 million of cancer related deaths was recorded 2.Gastric cancer (GC) ranks as the fourth most common cancer and the second leading cause of cancer death worldwide. According to a global estimation, approximately 985,600 new cases of gastric cancer are being diagnosed each year and a minimum of 738,000 patients are dying from the disease 3, 2, 4. Many factors are implicated in the development of gastric involving H. pylori infection, Epstein-Barr virus (EBV), chronic atrophic gastritis, previous gastric surgery, pernicious anemia, adenomatous polyps, prior radiation exposure and genetic factors 5.
Epstein-Barr virus is a DNA virus of the Gamma herpesvirinae family. Its entry route is via the oropharyngeal epithelium. After an initial incubation period in B lymphocytes, the virus begins to express its specific antigens and oncogenic characteristics 6. Epstein-Barr virus is associated with the transformation of various types of cells, such as lymphoid, dendritic, smooth muscle and epithelial cells, and 90% of the adults worldwide are infected, and most individuals carry the virus as a lifelong asymptomatic infection. EBV is associated with many human malignancies such as Burkitt’s lymphoma (BL), Hodgkin lymphoma (HD) and nasopharyngeal carcinoma (NPC) and about 10% of gastric carcinomas 7,8,9
Epstein-Barr virus after primary infection establishes the lifelong virus carrier state called latent infection, which expresses a limited set of viral genes 10, including Epstein-Barr nuclear antigens (EBNAs). They maintain the EBV genome in its episomal state and activate the transcription of viral, and cellular genes and Latent membrane protein 1 (LMP1) which interact with cellular proteins and intracellular signaling pathways. Both EBNAs and LMPs can be demonstrated in most EBV-associated cancers 11, 7. The aim of the present study was to determine the association between EBV and gastric carcinoma among Sudanese patient in Khartoum state, Sudan.
Material and Methods
Specimen’s Collection
50 Paraffin embedded blocks of gastric biopsy specimens were diagnosed as gastric carcinoma collected from April to May 2016 at the department of histopathology, Soba university hospital and Ribat teaching hospital, Sudan. Tissue sectioning was performed in (3μm) thickness to perform DNA extraction and polymerase chain reaction (PCR) for EBV detection. Basic information of the Patient were collected from patients’ records includes age, sex, clinical feature and histological type of the tumor.
Pretreatment for Paraffin-Embedded Tissue
About 20 mg of paraffin-embedded tissue was add to 1ml of xylene in an eppendorf tubes, vortex for 1min the tissue became transparent while paraffin remain white and then centrifuged at 13,000 rpm for 10 min. Supernatant was removed carefully with automatic pipette, each 1ml of samples of different concentration of ethanol such as 100%, 90%, 80%, 70% and 50%.After that added vortex for 1minand again centrifuged for 1min at 13,000 rpm. The supernatant was discarded without removing the pellet and was dried using filter paper, and then the open tube was incubated at 65C0 for 10-15 min for evaporation. Finally PBS was added to pellet and incubated overnight.
Molecular detection of EBV
DNA was extracted from the pellet using the DNeasy Blood & Tissue Kit (50) (QIAGEN, Germany). DNA quality was measure by a Nanodrop 1000 apparatus. Epstein-Barr virus gene was detected by PCR using two primers from published data 12 as follows:
SL1, 5\-GGACCTCAAAGAAGAGGGGG-3\,
SL3, 5\-GCTCCTGGTCTTCCGCCTCC-3\.
The primers amplify and detect an 80 base pair region of the EBNA1 gene. 25 μl of reaction mixture containing 5 μl DNA sample, 5 μl Maxime PCR PreMix Kit (i-Taq) (iNtRON Biotechnology Inc., Korea), 1 μl of each forward and reverse primer, and 13 μl nuclease-free water .The conditions for PCR analyses were as follows: 94 C for 10 min (1 cycle); 95 C for 45 sec, 60 C for 45 sec, 72 C for 60 sec (35 cycles); 72 C for 10 min (1 cycle). After PCR amplification, PCR products were analyzed by electrophoresis in a 2% agarose gel stained with safe stain (sinaclon-Iran) and observed under UV transillumination.
Statistical Analysis
Statistical analysis was done using the SPSS computer program (version 20: SPSS, Chicago, IL, USA). The Pearson chi-square was applied to examine the relationship between Epstein-Barr virus and gastric carcinoma.
Results
Clinical Features Associated with EBV Infection
Fifty gastric carcinoma samples collected from Soba University Hospital and Ribat Teaching Hospital during April and May 2016 included 43(86.0%) endoscopic biopsy and 7(14.0%) gastrectomy samples. Twenty seven (54.0%) of the gastric carcinoma patients were males and 23(46.0%) were females Table 1.
Table 1. Relation between EBV and the Gender of patient| Gender | Total | PCR | P- value | |
| Positive % | Negative% | |||
| Male | 27 | 8 (72.7%) | 19 (27.3 %) | 0.158 |
| Female | 23 | 3 (27.2%) | 20 (72.8 %) | |
| Total | 50 | 11 | 39 | |
The mean age of the patients was 56 years, and the most frequent age group was (50-59) years representing (34%) Table 2.
Table 2. Relation between EBV and Age of the patients| Age group | Total | PCR -ve | PCR+ve | P value |
| 40-49 | 14 (28) | 11 | 3(27.3) | |
| 50-59 | 17(34) | 11 | 6(54.5) | |
| 60-69 | 13 (26) | 13 | 0(0) | |
| 70-80 | 6 (12) | 4 | 2(18.2) | 0.118 |
| Total | 50 | 39 | 11 |
The most prominent clinical symptoms associated with EBV infection were gastritis, weight lost and anemia represents (63.6%) for each, anorexia (27.2%), and abdominal pain (9%) Figure 1.
Figure 1.Clinical features associated with EBV infection associated with Gastric Carcinoma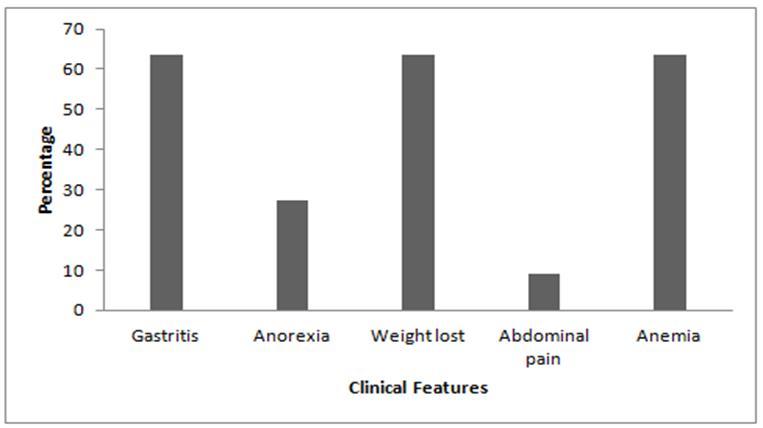
The clinical pathological findings among positive specimen showed that (30%) was poorly differentiated carcinoma and (20%) was mucinous carcinoma, while - well differentiated carcinoma, well differentiated adenocarcinoma, adenocarcinoma, signet ring, linitis plastic are equally distributed represented (10%) Figure 2.
Figure 2.Histopathological features of Epstein - Barr virus associated with Gastric Carcinoma
Molecular Detection of EBV
The gastric carcinoma samples were tested for EBV genome by PCR. Eleven (22.0%) EBV positive samples were found in the gastric carcinomas, 8 (72.7%) were from endoscopic biopsy and 3 (27.2%) were from gastrectomy, while 39(78%) were negative Figure 3.Among the positive sample 8 (72.7%) were males and 3(27.2%) were females Table 1. Similarly among the positive samples 6(54.5%) were at 50-59 year old Table 2. Most of the positive cases were (10%) from Khartoum, while (6.0%) were found from northern and western Sudan Figure 4.
Figure 3.PCR Results of EBNA1 gene in patients with Gastric carcinoma Lanes 1 is control negative for EBV gene. Lane 2 visualized PCR negative. Lane 3 clear band is visualized (positive PCR result) for EBV gene, Lanes 4 is control positive for EBV gene. M: 50 bp DNA size markers on 2% agarose gel.
Figure 4.Distribution of EBV positive gastric carcinomas by region
Discussion
Diet, smoking, alcohol intake, previous gastric surgery, and some gastric diseases, such as pernicious anemia, gastritis and Helicobacterpylori infection, are considered to be risk factors for the development of cancer 13. In the present study we found exists an association between EBV and gastric carcinoma in some Sudanese patients). In Tunisia 14.8% (12 out of 81) of GC cases were associated with EBV 14 and similarly 36% from Ninety-six GC cases were associated with EBV 15.Another study conducted in Sudan by Mahmoud etal showed that 7 of 30(23.3%) EBVaGC 16.
Several studies also showed significant association 17, 18, 19. However, Mouni 15indicated that EBV is not an important etiological factor in GC arising in North African populations.
Consistent to the previous studies males showed higher risk of infection compared to females 20,21, meta-analysis of 15,952 cases shown that EBV-positive in GC occur more frequently in male than in female patients 22. Most studies indicated that lifestyle or occupational factors may exist among males 10, 23, 24.The highest incidence of EBV in Gastric cancer was at (50-59) year age 21, 25 Occurrence in elderly persons and male predominance are common in EBV-associated gastric carcinomas 26. Gastritis, weight lost, anemia represents the most prominent clinical features (63.6%) among EBVaGC. Poorly differentiated carcinoma showed higher percentage representation (30%) among all histological findings of EBVaGC followed by mucinous gastric carcinomas(20%) , well differentiated carcinoma, well differentiated adenocarcinoma, adenocarcinoma, signet ring, linitis plastic representing the lowest percentage (10%) 27,28.
Three patients were first diagnosed by endoscopic biopsy showed no evidence of malignancy, but after one to two months they have been diagnosed again as poorly differentiated carcinoma and that may clarify the importance of PCR analysis for EBV. Although in situ hybridization method is more sensitive than PCR,We were forced to use PCR technique instead of it due to non availability of resources required for performing that method in our country.
In the present study we focus on EBNA-1 detection because it’s only viral protein that is consistently expressed in all types of EBV-associated malignancies, where it’s essential for the replication and stable persistence of EBV episomes, many evidences demonstrated that EBNA-1 alters the cellular environment to promote genomic instability and act as an oncogene 29,30.Whereas LMP1 was reported as the major oncogenic factor of nasopharyngeal carcinoma (NPC) development and was detected in 80%- 90% of NPC tumors 31, 32. This indicates that, these proteins are essential for EBV to immortalize B cells and to transform other types of cells, such as rodent fibroblasts, by changing transcription and sustainable activation of the cell signaling pathway 33. Our study focuses on the prevalence of EBVaGC, so there is no data on patients follow up however it is very useful in further study.
Conclusion
In the present study, we conclude that the prevalence of EBV in GC in Sudanese patients was higher than that reported in some previous studies. The highest positive cases were detected in male and that may be due to life style.
Acknowledgements
The authors acknowledge the staff of histopathology at Soba university hospital and Ribat teaching hospital for providing tissues for this study. And Ms. Gisma ahmed eisa for advice on SPSS analysis.
References
- 1. (2008) World Health Organization.The Global Burden of Disease: 2004Update.Geneva:World Health Organization.
- 2.Bernard W, Christopher P Stewart.Wild,World Cancer Report(2014)Published by the International Agency for Research on Cancer,Geneva. 31.
- 3.Joseph B Mabula, Mabula D Mchembe, Koy Mheta, Phillipo L Chalya, Massaga Fabian et al.Nestory Masalu and Hyasinta Jaka, Gastric cancer at only a university viral teaching protein hospital in northwestern that is Tanzania: a retrospective review of 232 cases, World essential Journal of Surgical for Oncology the2012,replication 10:. 257.
- 4.Yan Xinyu, Wang Kan, Lu Wenting, Qin Weijian, Cui Daxiang et al. (2016) CdSe/ZnS Quantum Dot-Labeled Lateral Flow Strips for Rapid and Quantitative Detection of Gastric Cancer Carbohydrate Antigen 72-4, Nanoscale Research Letters.11:. 138.
- 5.Boysen T, Friborg J, Stribolt K, Hamilton-Dutoit S, Goertz S et al.(Dec1,2011) Epstein-Barr virus-associated gastric carcinoma among patients with pernicious anemia. , International Journal of Cancer 129(11), 2756-60.
- 6.Epstein M A, Achong B G, Barr Y M. (1964) Virus particles in cultured lymphoblasts from Abdennadher Burkitt’s Lancet. 1, 702-703.
- 7.Xiao Feng Wang, Liang Hua, Li Ping Yan, Huang Bao-Hua, Luo Bing et al. (2005) Expression of Epstein-Barr virus genes in EBV-associated gastric carcinomas,World. , Journal of Gastroenterology 11(5), 629-633.
- 8.Liu Shuzhen, Zhao Zhenzhen, Han Lu, Liu Song, Luo Bing.(February9,2016) Epstein-Barr Virus Infection in Gastric Remnant Carcinoma and Recurrent Gastric Carcinoma in Qingdao of Northern China. , PLoS ONE 11(2), 1-13.
- 9.Uozaki Hiroshi, Fukayama Masashi. (2008) Epstein-Barr Virus and Gastric Carcinoma – Viral Carcinogenesis through Epigenetic Mechanisms. , Int J Clin Exp Pathol 1, 198-216.
- 10.Iizasa Hisashi, Nanbo Asuka, Nishikawa Jun, Jinushi Masahisa, Yoshiyama Hironori. (2012) Epstein-Barr Virus (EBV)-associated Gastric Carcinoma.Viruses. 4, 3420-3439.
- 11.Kuratsune Hirohiko, Sairenji Takeshi, Fukuda Makoto, Kurosaki Wataru, Yanagihara Kazuyoshi. (2002) A Mechanism in Epstein–Barr Virus Oncogenesis: Inhibition of Transforming Growth Factor-_1-mediated Induction of MAPK/p21 by LMP1.Virology. 302, 310-320.
- 12.Mizobuchi Shunji, Sakamoto Hiromi, Tachimori Yuji, Kato Hoichi, Watanabe Hiroshi et al. (1997) . Absence of Human Papillomavirus-16 and -18 DNA and Epstein–Barr Virus DNA in Esophageal Squamous Cell Carcinoma. Jpn J Clin Oncol 27(1).
- 13.Bryan J, David L, Cass Carol, John R, Anil A Joy et al.(January2005) Hamilton, Gastric Adenocarcinoma Review and Considerations for Future Directions,Annals of Surgery. 241(1).
- 14.BenAyed-Guerfali Dorra.Wajdi Ayadi, Imen Miladi-Abdennadher, Abdelmajid Khabir, Tahia Sellami-Boudawara, Ali Gargouri, Raja Mokdad-Gargouri. (2011)Characteristics of epstein barr virus variants associated with gastric carcinoma in Southern Tunisia. , Virology Journal 8, 500.
- 15.Trimeche Mouni.Feriel Ksiâa, Sonia Ziadi, Sadok Korbi. (June2009) Prevalence and characteristics of Epstein-Barr virus-associated gastric carcinomas in Tunisia, European journal of gastroenterology and hepatology. 21(9), 1001-7.
- 16.Mohammed Mahmoud. (2016) Satti, 2Ibrahim Bakhit Yousif Elemam. Association of EBV in Gastric carcinoma among Sudanese patients,International Journal of Medical Science and Clinical Inventions 3(2), 1557-1559.
- 17.Camtu D Truong, Feng Wei, Li Wei, Khour T, Li Q et al. (2009) Characteristics of Epstein-Barr virus-associated gastric cancer: Astudy of 235 cases at a comprehensive cancer center in U.S.A. , Journal of Experimental & Clinical Cancer Research 28, 14.
- 18.Tang Weihua, Douglas R Morgan, Michael O Meyers, Ricardo L Dominguez, Martinez Enrique et al. Pei Fen Kuan, Natalie Banet, Hind Muallem, Kimberly Woodward, Olga Speck,and Margaret (2012) Epstein-barr virus infected gastric adenocarcinoma expresses latent and lytic viral transcripts and has a distinct human gene expression profile, Infectious Agents and Cancer7:. 21.
- 19.Xin Zu Chen, Chen Hongda, Felipe A, Hu Jian-Kun, Brenner Hermann et al.(May2015) Epstein–Barr Virus Infection and Gastric Cancern a Systematic Review. , Medicine 94(20).
- 20.Lee J H, Kim S H, Han S H, An J S, Lee E S et al.(Mar2009) Clinicopathological and molecular characteristics of Epstein-Barr virus-associated gastric carcinoma: a meta-analysis, journal of Gastroenterology and Hepatology. 24(3), 354-65.
- 21.Suminori Akiba.Chihaya Koriyama, Shan Ding, Edgardo Reyes, Tetsuhiko Itoh, Yoshie Minakami, Yoshito Eizuru, Roberto Herrera Goepfert. (2005).Epstein-Barr virus-associated gastric carcinoma: Evidence of age-dependence among a Mexican population. , World Journal of Gastroenterology 11(39), 6096-6103.
- 22.Murphy G, Pfeiffer R, Camargo M C, Rabkin C S. (2009) Meta-analysis shows that prevalence of Epstein-Barr virus-positive gastric cancer differs based on sex and anatomic location. , Gastroenterology 137(3), 824-33.
- 23.S1 Akiba, Koriyama C, Herrera-Goepfert R, Eizuru Y.(Feb2008) Epstein-Barr virus associated gastric carcinoma: epidemiological and clinicopathological features. , Cancer Science 99(2), 195-201.
- 24.Cho Junhun.Myung-Soo Kang, Kyoung-Mee Kim. (Mar2016) Epstein-Barr Virus-Associated Gastric Carcinoma and Specific Features of the Accompanying Immune Response. , J Gastric Cancer 16(1), 1-7.
- 25.Rymbai M L, V Ramalingam, Samarasan I, Chandran B S, Mathew G et al.(Jul-Sep2015).frequency of Epstein--Barr virus infection as detected by messenger RNA for EBNA 1 in histologically proven gastric adenocarcinoma in patients presenting to a tertiary care center in South India. , Indian journal of Medical Microbiology 33(3), 369-73.
- 26.Lopes L F, Bacchi M M, Elgui-de-Oliveira D, Zanati S G, Alvarenga CE M et al.. , (Nov2004)Brazilian Journal of Medical and Biological Research. Volume 37(11), 1707-1712.
- 27.Jong Sun Choi.Min A Kim, Hee Eun Lee, Hye Seung Lee, Woo Ho Kim. (August2009) Mucinous Gastric Carcinomas, Issue Cancer. Volume 115, Issue 15. 3581-3590.
- 28.Schauer M, Peiper M, Theisen J, Knoefel W. (2011) Prognostic factors in patients with diffuse type gastric cancer (linitis plastica) after operative treatment. , European Journal of Medical Research 16(1), 29-33.
- 29.Shinozaki-Ushiku Aya.Akiko Kunita, Masashi Fukayama.(2015).Update on Epstein-Barr virus and gastric cancer (Review). , INTERNATIONAL JOURNAL OF ONCOLOGY 46, 1421-1434.
- 30.Saridakis Vivian, Sheng Yi, Sarkari Feroz, Melissa N, Rongguang G et al. (2005) . Structure of the p53 Binding Domain of HAUSP/USP7 Bound to Epstein-Barr Nuclear Antigen 1 Implications for EBV-Mediated Immortalization, Molecular Cell 18, 25-36.
- 31.Abdelwahid Saeed Ali, Al-Shraim Mubarak, Ahmed Musa Al-Hakami, Ian M Jones. (2015) Epstein- Barr Virus: Clinical and Epidemiological Revisits and Genetic Basis of Oncogenesis. , Open Virology Journal 9, 7-28.