
The Risk Factors, Complications, Management Strategies and Predictors of Morbidity & Mortality Among Pediatric Patients Presenting with Severe Diarrhea at Muhimbili National Hospital’s Emergency Medicine Department
Abstract
Background
Acute diarrhea is the major cause of health public problem among paediatric patients in Tanzania. And in Low income countries (LICs), studies have shown, Acute watery Diarrhea (AWD) is the cause of morbidity and mortality which can be prevented by immediate identification and treatment of complications.
Methods
A prospective cohort study was done between December 2021 and April 2022 to determine the risks, complications, management strategies and predictors of mortality among paediatric patients ≤12 years of age with severe diarrhea. We excluded those who arrived in cardiac arrest at the Emergency Medicine Department (EMD) of Muhimbili National Hospital (MNH). Proportion was used to summarize the counts and frequency of participants who were at risk of complications and management strategies given and for predictors of outcomes. A Modified Poisson log linear model with a robust estimation test was used to test for significant associations between predictors and outcomes. Multivariate logistic regression was used to adjust for confounders.
Results
A total 6,570 paediatric patients presented to EMD during study period, and we recruited 144 (2.2%). The median age was 1 (IQR 0.7-2.0) years and most were male 86 (59.7%). Among the study participants with diarrhea, 120 (83.3%) had dehydration, acidosis 60 (42.3%), hypoglycemia 8 (5.6%), hypokalemia 76 (53.1%), and Acute renal failure 11 (7.6%). Those patients with complications received appropriate management, including IV crystalloid solution given to 131 (90.97%), and correction of acidosis 60 (42.3%), hypoglycemia correction with IV dextrose 10% 6 (4.2%), and hypokalemia and infections were corrected with IV potassium chloride 52 (36.1%) and IV antibiotic treatment 84 (58.3%) respectively.
Conclusion
Pediatric patients under 2 years of age are at high risk of severe diarrhea with dehydration as compared to other ages. Early referral and availability of point care tests are essential in early recognition of accompanied complications.
Article Information
- Received
- Accepted
- Published
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Manyasani Jisoli Yahula, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Manyasani Jisoli Yahula, Emergency Medicine Department, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania —
Competing Interests
The author declares no conflict of interest
Funding
This was a non-funded project; the principal investigators used their own funds to support the data collection and logistics
Data Availability
The data set supporting the conclusion of this article is available from the authors on request
Acknowledgements
The author would like to thank all the study participants, Mr Francis Ambrose and all other research team, Mr Peter, for all the assistance in making this project a success.
Citation:
Introduction
The burden of diarrheal disease seriously affects young children in developing countries, where incidence rates are high due to inadequate purification of water, poor sanitation, suboptimal breastfeeding, as well as zinc and vitamin A deficiency. Vulnerable children living in impoverished, undeveloped areas and rural areas have higher fatality rates compared to children living in developed and planned urban areas due to lack of access to quality health care, timely intervention, and effective treatment with oral rehydration solution (ORS) and zinc 1, 2, 3.
The loss of water and electrolytes from the body in liquid stool causes the acute effects of acute diarrhea that prompt EMD visits. Additional amounts of water and electrolytes are lost when there is vomiting, and water losses are also increased by fever. These losses cause dehydration (due to the loss of water and sodium chloride), metabolic acidosis (due to the loss of bicarbonate), and potassium depletion. Dehydration, if left untreated, promptly becomes the most dangerous condition because it can cause decreased blood volume (hypovolemia), cardiovascular shock, and death 4.
Diarrhea in children is one of the major causes of malnutrition, stunting and mortality among children under-five years of age worldwide; particularly in developing countries. Every year, diarrhea kills around 525,000 children under five years of age. Globally, there are nearly 1.7 billion cases of childhood diarrhea disease every year 12.
The Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhea (GAPPD) proposes a mechanism through involvement of parents, communities, community health workers (CHWs), civil society and private sectors towards ending children′s death from pneumonia and diarrhea 10.
At primary and secondary hospitals, the management of acute diarrhea disease is based on the Integrated Management of Childhood Illnesses (IMCI) guidelines through following these five recommendations, use of vitamin A, oral rehydration solution, elemental zinc, ciprofloxacin for blood diarrhea in all HIV infected and exposed infants and daily use of micronutrients 7, while at EMD life threatening complications such as dehydration, electrolyte imbalances, acidosis, hypoglycemia, acute renal failure and leukocytosis are primarily fixed first at EMD of MNH.
Several studies in Tanzania have revealed that diarrhea is a major public health problem among children under the age of five. Despite public health initiatives, treatment advances, and improved diagnostic tools, acute diarrheal illness remains one of the two leading causes of death in the paediatric population. Health facility reports in 2015 indicated that diarrhea is one of the top five causes of mortality among under five children in Tanzania 8.
The national survey-based study done in Tanzania in 2015-2016 reported the overall prevalence of childhood diarrhea for under five children was 12.1% 9. The reported prevalence of diarrhea varies over a very wide range (from 2 to 95%) 10. For example, in a survey done among nurses who were asked to inspect feces, they agreed on the presence or absence of diarrhea on only 75% of the occasions 11. To have a standard definition of diarrhea, the ‘Bristol Stool charts’ are used 12.
Physicians operating in emergency settings are frequently faced with the challenge of treating children with acute diarrhea and should be prepared to make evidence-based diagnostic and treatment decisions 13.
This study will help to determine the risk factors, identify the complications, and identify the management strategies needed to prevent poor outcomes (morbidity and mortality) at EMD and after 24hours among paediatric patients presenting with severe diarrhea at the EMD of MNH.
The study hypothesis
The risk factors including age less than 2 years, malnutrition, delayed referral, and hypokalemia are significantly associated with increased morbidity and mortality among paediatric patients presenting with severe diarrhea at Muhimbili National Hospital’s Emergency Medicine Department.
Methodology
Study design
This was a prospective cohort study of paediatric patients presenting with severe diarrhea at EMD MNH and followed for outcomes at EMD and after 24-hours.
Study area
The study area was at the EMD of MNH in Dar-es-Salaam, Tanzania and all the pediatric wards at MNH and Pediatric Intensive Care Unit (PICU) where patients’ data was traced for 24-hours follow-up. MNH is located in Ilala district, along Malik Road, in Upanga. MNH has a bed capacity of 1500 and serves as the top referral hospital in Tanzania. The EMD was established in 2010 via a partnership between the Ministry of Health and Social Welfare and the Abbott Fund Tanzania. The EMD is the first full capacity public Hospital in Tanzania and currently the only training site for emergency medicine residency program in the country.
The department is staffed 24 hours, seven days a week by locally trained specialist emergency physicians, who oversee the care of patients and training of interns, registrars and emergency medicine residents. The pediatric patients are seen in pediatric wing D, where stabilization is done before disposition to the ward. The department receives about 90 pediatric patients with acute diarrhea and related complications per month. The age limits of paediatric patients seen at EMD are those who are 12 years and below. Those who are 12 years above are attended as adult patients, hence the age limit for this study was adopted based on the hospital age limit criteria for easy tracking and follow-ups. There is one machine in the EMD for electrolyte testing and acid base disorders, as well as diagnostic imaging, including portable x-ray and point of care ultrasound, fluids, antibiotics, two ventilator machines with airway devices, one CT scan machine accessible for all patients and laboratory services. The EMD has 19 emergency medicine specialists who attend patients yearly.
The target population
All paediatric patients presenting with severe diarrhea at EMD MNH, Tanzania
The accessible population were the paediatric patients with severe diarrhoea attending EMD MNH.
The study population
All paediatric patients twelve years of age and below presenting with severe diarrhoea at EMD MNH during the study period.
Sample size estimation
The estimation of sample size was based on a study conducted in Nigeria by Okoronkwo et al on “Pattern of morbidity and mortality of childhood illnesses at children′s emergency room of Abia State University Teaching Hospital: a descriptive prospective study” that reported 10.5% of deaths at the emergency room among paediatric patients were due to acute diarrhoea (14). This proportion and other assumptions (confidence interval (Cl=95%), Z=1.96 and margin error (Ɛ) =5% were used to calculate the sample size in this study. Therefore, in consideration of the study done, the sample size was calculated by the formula below;
Formula
N=Z²P (1-P)/ Ɛ²
Where
N=sample size
Z=standard normal deviate at 95% confidence interval
P= mortality of 10.5% among pediatric patients with acute diarrhea death at the emergency room.
Ɛ=tolerable error 0.05
Substituting for the formula above
N=1.96² *10.5(100-10.5)/5²
N=144
The estimated sample size of pediatric patients with acute diarrhea presented at MNH EMD for this study was 144
Sampling Design
A simple random sampling technique was used
Selection criteria
Inclusion criteria
All paediatric patients 12years of age and below, who presented with severe diarrhea at EMD, MNH during the study period and the study participants whose caregivers/guardians agreed to give consent for participation in the study
Exclusion criteria
All Pediatric patients who were critically ill and arrived in cardiac arrest at EMD and Cardiopulmonary resuscitation done and those who were lost to follow up
Variables
Independent variables
This included the age and gender of the study participant, the location of the home of the study participant (region, district, ward, and street), the age of the guardian/care giver, the source of water for cooking and drinking, the clinical presentation on arrival, (such as level of consciousness measured as AVPU, heart rate, work of breathing, and capillary refills abnormalities associated with severe diarrhea such as hypokalemia, and acidosis, and the management done at EMD MNH.
Dependent variables
EMD morbidity and mortality, dehydration and 24 hours′ outcomes (disposition to PICU, pediatric ward or discharged home for outpatient care) and their status at 24 hours were traced for continuity of care. Note, dehydration was determined using a WHO flowchart for assessing hydration status; ASK: What about for how long has the child had diarrhea? Ask: Is there blood in the stool? Look at the child's general condition. Is the child lethargic or unconscious? Restless and irritable? Look for sunken eyes, offer the child fluid. Is the child not able to drink or is drinking poorly? Drinking with zeal and thirst? Pinch the skin of the abdomen. Does it go back? Very slowly (longer than 2 seconds)? Slowly? Classify the child's dehydration as severe dehydration if it has two or more of the following: Lethargic or unconscious, sunken eyes, not able to drink or drinking poorly, skin pinches go back very slowly (longer than 2 seconds). Some dehydration if you have two or more of the following: restless, irritable, sunken eyes, drinking eagerly, thirsty, skin pinching goes back slowly (less than 2 seconds but longer than normal) and there is no dehydration if two or more of the signs of some dehydration are not present 15.
Study outcomes
Primary outcome
24hrs mortality at EMD: this includes death while at EMD or in the ward or PICU within 24hours.
Secondary outcome
The risks of acquiring severe diarrhoea, complications-such as electrolyte imbalances, acid base abnormality and dehydration status, management strategies of the complications at EMD, and predictors of outcomes.
Data collection method
Data collection
Data collection was done by the principal investigator, with the assistance of a research assistant, who was a medical doctor, and was trained on how to recruit patients based on the inclusion and exclusion criteria, during data collections and enrolment, study participants were assigned numbers from the study population meeting the study criteria, and the numbers were put in box, then numbers were randomly picked every day, and those participants who whose their numbers were picked were interviewed as per questionnaire after consenting for the study and the information obtained were filled correctly in the questionnaire, the study assistant was assisted wherever necessary, until the estimated sample size was reached.
The stool was observed for assessment using the full scale, Bristol stool chart for diagnosis of diarrhoea 12. If the stool was not produced, the caregiver was shown the Bristol stool chart to identify the stool that, the child has been passing. Through a structured questionnaire, information such as social demographic features, clinical profile, and assessment of different risk factors for diarrhoea was gathered.
Study participants were followed up after disposition, where outcomes such as EMD complications, morbidity & mortality and 24-hour mortality were recorded.
The diagnosis of diarrhea was made by using the patient's history and the Bristol stool full form scale. The patient who had type 5 to 7 was regarded to have diarrhea as per Bristol stool.
Data analysis plan
Data obtained was de-identified, coded, cleaned, and entered into the Statistical Package for Social Science (IBM SPSS version 25, IBM, LTD, Carolina, USA). Data was then summarized in the form of proportions and frequency tables for categorical variables. Mean, median with inter quartile range and proportions were used to summarize continuous variables. A Modified Poisson log linear model was used to test for the significance of associations between the predictors and outcome variables for continuous variables. Multivariate logistic analysis was used to determine the categorical predictor variables that are associated with the outcome. Significance was defined as a p-value of less than 0.05. In addition, subgroup analyses were done for age categories < 2 years, 2-5 years and > 5 years but less or equal to 12 years, age of care takers < 25years, 26 – 35 years and > 35 years, duration of passing stool per day; < 5 days and ≥ 5 days and frequency of passing stool per day; < 4 frequency per day and ≥ 4 frequency per day
Objective number 1. To determine the risk factors for acquiring severe diarrhea that were present among pediatric patients presenting to the EMD MNH from December 2021 to April 2022. The number/proportion of patients with each risk factor was analyzed with frequency.
Objective number 2. To describe the complications of severe diarrhea among pediatric patients presenting at EMD MNH from December 2021 to April 2022.
The complications were analyzed using the frequency of any complication from severe diarrhea.
Objective number 3. To describe the management strategies of severe diarrhea among pediatric patients presenting at EMD MNH from December 2021 to April 2022.
The management strategies of severe diarrhea among pediatric patients presenting at EMD MNH were analyzed using frequency
Objective number 4. To determine the predictors of morbidity & mortality from severe diarrhea among pediatric patients attending EMD MNH from December 2021 to April 2022.
The predictors of morbidity and mortality from severe diarrhea among pediatric patients attended at EMD MNH were analyzed using a modified poison log linear regression model and logistic regression.
Ethical consideration
Ethical approval for this study was obtained from the Muhimbili University of Health and Allied Sciences Institutional Review Board, Approval No. MUHAS-REC-02-2022-951.
Results
Flow diagram of paediatric patients with AWD attended at EMD MNH, Tanzania
A total of 6,570 paediatric patients were attended at EMD MNH during the study period. There were 164(2.50%) paediatric patients with severe diarrhoea. Of all patients, twenty (12.20%) among those who met the criteria had missing information and 144(87.80%) were enrolled and all were able to be followed up for 24 hours (Figure 1).
Figure 1. Flow diagram of paediatric patients with AWD attended at EMD MNH, Tanzania.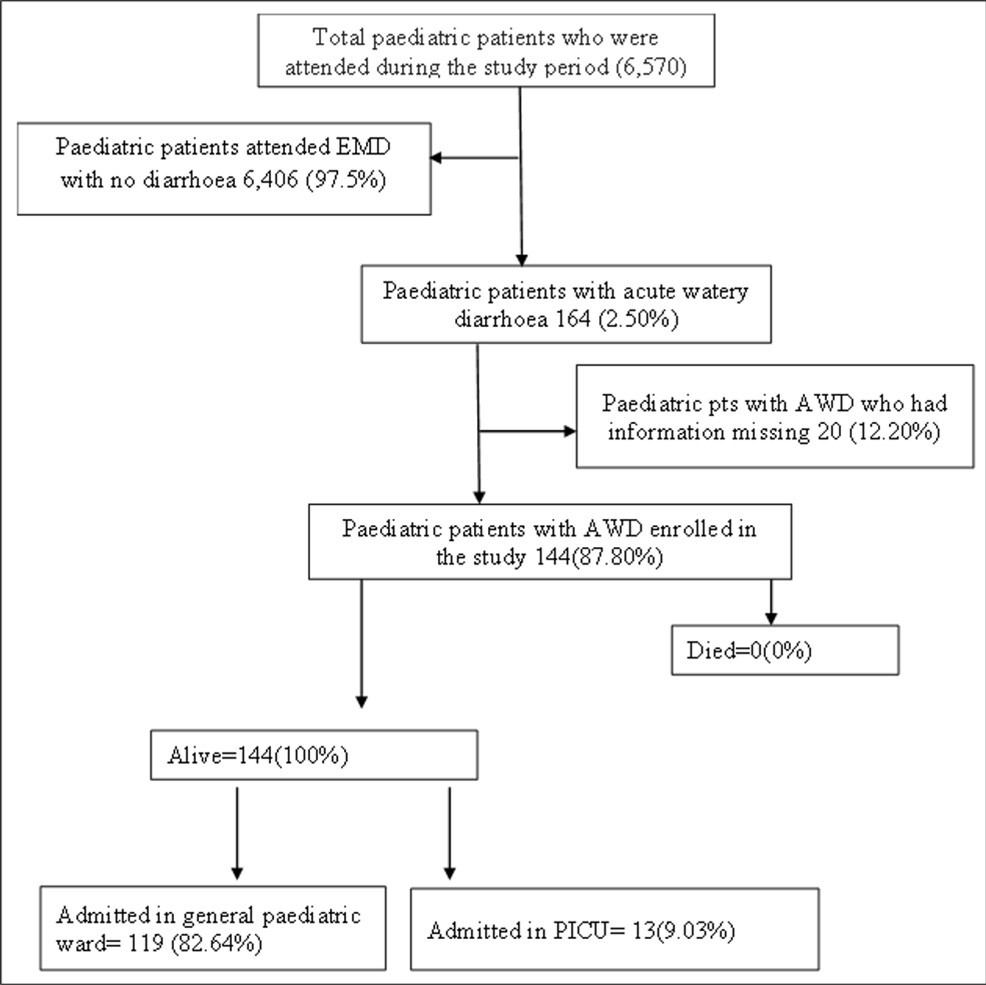
Download figure
Sociodemographic characteristics of the study participants
Among 144 paediatric patients with severe diarrhoea who were attended at EMD MNH, the median age was 1 (IQR 0.7, 2.0) years, 86 (59.7%) were male and most of the study participants were under 2 years of age 103 (70.8%). Of all study subjects’ majority 137 (95.1%) had been exclusively breastfed for 6 months or longer, 125 (86.80%) were from Dar es Salaam, and 92 (63.90%) were referred cases. The primary caretaker aged between 26 and 35, married in most cases, and 87.5% had completed secondary school (Table 1).
Table 1. Socio demographic characteristics of study participants| Variable | Frequency (n) | Percent (%) |
|---|---|---|
| Age of the children (years) | ||
| < 2 | 102 | 70.8 |
| 2 - 5 | 26 | 18.1 |
| >5 | 16 | 11.1 |
| Median age of the children in years (IQR) | 1 (0.7, 2.0) | |
| Sex of the child | ||
| Male | 86 | 59.7 |
| Female | 58 | 40.3 |
| Duration of Exclusive Breast Feeding (EBF) | ||
| Less than 6 months | 7 | 4.9 |
| Completed EBF | 137 | 95.1 |
| Age group of caretakers (years) | ||
| < 25 | 14 | 9.7 |
| 26 – 35 | 96 | 66.7 |
| >35 | 34 | 23.6 |
| Median age of caretaker in years (IQR) | 31 (29, 35) | |
| Residence | ||
| Dar es salaam | 125 | 86.8 |
| Outside Dar es salaam | 19 | 13.2 |
| Referral status | ||
| Hospital referral | 92 | 63.9 |
| Self-referral | 52 | 36.1 |
| Health insurance status | ||
| Not Insured | 94 | 65.3 |
| Insured | 50 | 34.7 |
| Mother or caregiver level of education | ||
| Completed Primary school | 9 | 6.3 |
| Completed Secondary school | 126 | 87.5 |
| College/University | 9 | 6.3 |
| Partner education level of caregiver | ||
| No formal education | 1 | 0.7 |
| Secondary | 143 | 99.3 |
| Employment status | ||
| Not employed | 6 | 4.2 |
| Self-employed | 117 | 81.3 |
| Public | 7 | 4.9 |
| Private employed | 14 | 9.7 |
| Marital status | ||
| Married | 133 | 92.4 |
| Widow | 2 | 1.4 |
| Separated/divorced | 9 | 6.3 |
The children and environmental characteristics related to severe diarrhoea; most of the children were using tap as drinking water, only 13 (9.0%) reported using antibiotics 7 -14 days prior to severe diarrhoea, 102 (70.8%) had passage of loose stool more than 5 days and with 95 (66.0%) with 4 or more stools per day (Table 2).
Table 2. Children and environmental characteristics in paediatric participants with acute diarrhoea.| Variable | Frequency (n) | Percent (%) |
|---|---|---|
| Source of drinking water | ||
| Tap/Municipal | 143 | 99.3 |
| Well | 1 | 0.7 |
| Number of under-five dwells in the house | ||
| 0 - 1 | 100 | 69.5 |
| 2 | 39 | 27.1 |
| 3 | 5 | 3.5 |
| Neighbor child with diarrhea | ||
| Yes | 21 | 14.6 |
| No | 121 | 84.0 |
| Not sure | 2 | 1.4 |
| Use of antibiotics before onset within 7-14 days | ||
| Yes | 13 | 9.0 |
| No | 131 | 91.0 |
| Duration of passing loose stool (days) | ||
| < 5 | 102 | 70.8 |
| ≥ 5 | 42 | 29.2 |
| Frequency of passing loose stool | ||
| < 4 | 49 | 34.0 |
| ≥ 4 | 95 | 66.0 |
Factors associated with dehydration among paediatric patients with severe diarrhoea
Most of the paediatric patients with dehydration were under 2 years of age 91 (89.2%) among the paediatric participants which it was statistically significant with p-value of 0.036, and 114 (83.2%) had completed breast feeding for 6 months, though it was not statistically significant, 103 (81.7%) completed secondary school, majority of care givers were between 26-35 years of age 77 (80.3%), most of paediatric patients did not reports use of antibiotics 110 (84.0%) prior to onset of severe diarrhoea, 82 (80.4%) had passage of loose stool for less than 5 days and 82 (86.3%) had more or equal to 4 motion of loose stool per day, all these were not statistically significant (Table 3).
Table 3. Factors associated with dehydration among paediatric patients with severe diarrhoea| Variable | Acute watery diarrhea | ||
|---|---|---|---|
| No dehydration | dehydration | p-value | |
| Age of the child (years) | |||
| < 2years | 11 (10.8) | 91 (89.2) | 0.036 |
| 2-5 years | 9 (34.6) | 17 (65.3) | |
| >5years | 4 (25.0) | 12 (75.0) | |
| Durations of EBF | |||
| < 6months | 1 (14.3) | 6 (85.7) | 0.850 |
| Completed 6months | 23 (16.8) | 114 (83.2) | |
| Care giver level of education | |||
| College/university | 0 (0.0) | 9 (100.0) | 0.072 |
| Completed secondary school | 23 (18.3) | 103 (81.7) | |
| Completed primary school | 1 (11.1) | 8 (88.8) | |
| Age of care giver (years) | |||
| ≤ 25years | 1 (7.1) | 13 (92.8) | 0.369 |
| 26 - 35years | 19 (19.8) | 77 (80.3) | |
| >35years | 4 (11.8) | 30 (88.2) | |
| Partners education level | |||
| No formal education | 0 (0.0) | 1 (100.0) | 0.361 |
| Secondary school | 24 (16.7) | 119 (83.2) | |
| Use of antibiotics before onset 7 - 14 days | |||
| Yes | 3 (23.1) | 10 (76.9) | 0.639 |
| No | 21 (16.0) | 110 (84.0) | |
| Duration of passing loose stool | |||
| < 5 days | 20 (19.6) | 82 (80.4) | 0.140 |
| ≥ 5 days | 4 (9.5) | 38 (90.5) | |
| Frequency of passing loose stool | |||
| < 4 | 11 (22.4) | 38 (77.6) | 0.181 |
| ≥ 4 | 13 (13.7) | 82 (86.3) | |
Complications of paediatric patients presenting with severe diarrhoea at EMD MNH
Most of the participants, 120 (83.3%) had dehydration among the paediatrics with acute diarrhoea, electrolyte imbalances-hypokalaemia was 76 (53.1%), acute renal failure contributed to 11 (7.6%) among 144 paediatric patients, leucocytosis had 16 (11.2%) paediatric patients and 8 (5.6%) had hypoglycaemia, most patients had point of care venous blood gases were done as an investigation to rule out electrolytes imbalances and monitor treatment outcomes, point of care random blood glucose, creatinine and urea and full blood count which were sent to central laboratory (Table 4).
Table 4. Complications of severe diarrhoea among paediatric patients presented at EMD MNH| Variable | Variable | Frequency (n) |
|---|---|---|
| Dehydration status | ||
| No dehydration | 24 | 16.7 |
| Some dehydration | 92 | 63.9 |
| Severe dehydration | 28 | 19.4 |
| Hypokalemia | ||
| Yes | 76 | 53.1 |
| No | 67 | 46.9 |
| Acidosis | ||
| Yes | 60 | 42.3 |
| No | 82 | 57.7 |
| Acute renal failure | ||
| Yes | 11 | 7.6 |
| No | 133 | 92.4 |
| Leukocytosis | ||
| Yes | 16 | 11.2 |
| No | 127 | 88.8 |
| Hypoglycemia | ||
| Yes | 8 | 5.6 |
| No | 136 | 94.4 |
Management strategies of severe diarrhoea among paediatric patients with severe diarrhoea at emergency medicine department of Muhimbili National Hospital
Management strategies that were used by the study participants. Among 144 paediatric patients, 131 (90.97%) were given IV crystalloids, IV potassium chloride for correction of hypokalaemia 52 (36.1%), IV dextrose 10% was given to 6(4.2%) for corrections of hypoglycaemia., and IV antibiotics was given to 16(11.2%) of the study participants (Table 5).
Table 5. Management strategies of severe diarrhoea given at EMD| Variable | Frequency (n) | Percent (%) |
|---|---|---|
| IV Crystalloid solution given | ||
| Yes | 131 | 90.97 |
| No | 13 | 9.03 |
| Potassium chloride, (KCL) given | ||
| Yes | 52 | 36.1 |
| No | 92 | 36.1 |
| IV Dextrose 10% given | ||
| Yes | 6 | 4.2 |
| No | 138 | 95.8 |
| IV antibiotic given | ||
| Yes | 84 | 58.3 |
| No | 127 | 88.8 |
Univariate and multivariate analysis of potential predictors of disposition outcomes
Dehydration, hypokalemia, Acidosis, Hypoglycemia, Acute renal failure, Anemia, Leukocytosis, abnormal nutrition status, Duration of diarrhea, and referral status were all found be predictors of admission to the ward or Pediatric ICU in the univariate analysis, but in the multivariate analysis, only hypokalemia and referral status were found to be independent predictors of severe diarrhea among paediatric participants in in this study (Table 6).
Table 6. Univariate and multivariate analysis of the factors associated with severe diarrhea.| Variable | Category | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|---|
| cPR | 95% CI | P - value | aPR | 95% CI | P - value | ||
| Dehydration | Yes | 1.34 | 1.03 – 1.74 | 0.027 | 1.19 | 0.91 – 1.56 | 0.204 |
| No | Ref | ||||||
| Hypokalemia | Yes | 1.24 | 1.10 – 1.40 | < 0.001 | 1.13 | 1.03 – 1.24 | 0.008 |
| No | Ref | ||||||
| Acidosis | Yes | 1.15 | 1.05 – 1.27 | 0.004 | 1.03 | 0.95 – 1.11 | 0.496 |
| No | Ref | ||||||
| Hypoglycemia | Yes | 1.11 | 1.05 – 1.17 | < 0.001 | 1.04 | 0.97 – 1.11 | 0.293 |
| No | Ref | ||||||
| Acute renal failure | Yes | 1.11 | 1.05 – 1.17 | < 0.001 | 0.97 | 0.91 – 1.04 | 0.372 |
| No | Ref | ||||||
| Anemia | Yes | 1.17 | 1.02 – 1.34 | 0.027 | 1.02 | 0.88 – 1.18 | 0.800 |
| No | Ref | ||||||
| Leukocytosis | Yes | 1.11 | 1.05 – 1.18 | < 0.001 | 1.07 | 0.98 – 1.18 | 0.132 |
| No | Ref | ||||||
| Abnormal nutrition status | Yes | 1.11 | 1.05 – 1.17 | < 0.001 | 1.04 | 0.96 – 1.13 | 0.363 |
| No | Ref | ||||||
| Duration of diarrhea(days) | ≥ 5 | 1.15 | 1.06 – 1.23 | < 0.001 | 1.05 | 0.99 – 1.11 | 0.095 |
| < 5 | Ref | ||||||
| Frequency of passing loose stool | ≥ 4 per day | 1.06 | 0.94 – 1.19 | 0.373 | 1.03 | 0.92 – 1.16 | 0.596 |
| < 4 per day | Ref | ||||||
| Referral status | Hospital | 1.28 | 1.10 – 1.48 | 0.001 | 1.15 | 1.01 – 1.30 | 0.025 |
| Self | Ref | ||||||
24 hours’ outcomes for paediatric participants with severe diarrhoea
Among all the pediatric patients who were enrolled,144 were alive, 82.64% among them were admitted to the ward, 9.03% were admitted to PICU, and 8.33% were managed and discharged home, there were no deaths at EMD and after 24hours of following (Figure 2)
Figure 2. Pediatric participants with severe diarrhea attended at emergency medicine, followed until disposition and 24-hours of outcomes from EMD MNH.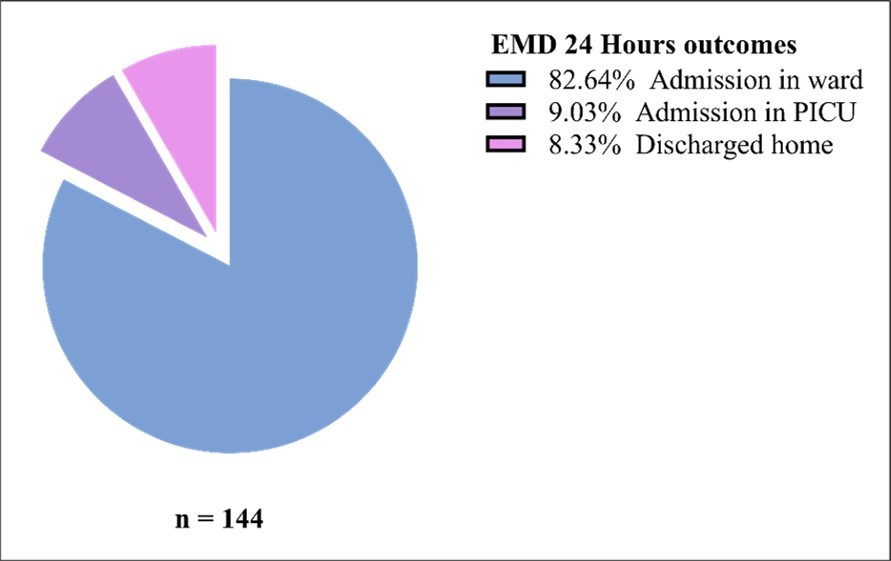
Download figure
Discussion
In this study, among the paediatric participants with severe diarrhoea attended at EMD MNH, majority of the study participants with severe diarrhoea complications were seen in under 2 years of age, as compared to other age groups, similar to other studies in LIC′s which have shown under 2 years have increased risks of acute diarrhea. Such as, the study done in Rwanda on the Risks factors associated with under 5 years of age diarrhoea and their effect on mortality, showed most of children affected were under 2 years of age, study done by Frederic Ndikubwimana et al from Rwanda 16, 17.
Also, the results in this study showed there were no deaths within 24 hours, which is different from the study conducted in Nigeria by Okoronkwo et al on the “Pattern of morbidity and mortality of childhood illnesses at children′s emergency room of Abia State University Teaching Hospital: a descriptive prospective study” that reported 10.5% of deaths at the emergency room among paediatric patients were due to acute diarrhoea 14, the differences can explained as results of this study, the outcomes was evaluated from 24 up to 48 hours stay at emergency. Also, of these paediatric participants, 119 (82.64%) among them were admitted in the ward,13 (9.03%) was admitted in PICU and 8.33 were discharged home after EMD management.
Referral from other hospital, this has been found in our study as there were 92 (63.9%) among pediatric patients with severe diarrhea were referred to the EMD MNH, in the univariate and multivariate analysis the referral status had statistical significant in determining outcomes for pediatric patients with severe diarrhea, similar to the study done at Malawi for pediatric patient under the age of five years were referred to tertiary level facility due inadequate emergency equipment’s like oxygen cylinders ,drugs and medical supplies etc. by Wezzie Kaunda et al 18 With regards to level of mothers’ education, in this study children who were born with the mothers who have secondary school level of education, 126 (87.5%) were found to have diarrhea more as compared to those who had primary school, (thus could state may be they are employed and leave their children with care givers at home (house girls to care) 9 (6.3%), similar to the study done by Paul Edwin et al 9
The most common electrolyte abnormality which was found in our study was hypokalaemia, which was seen in almost half of children and it was statistically significant in both univariate and multivariate analysis with the p-value < 0.05, used in determining the disposition of the paediatric patients in the ward (general ward and PICU), similar to the descriptive study done by Pratima P et al, where the mostly identified electrolyte imbalances were hyponatremia and hypokalaemia, with hypokalaemia observed in 21 (26.5%) and these were reported to be responsible for most death 17.
In this study, the management of severe diarrhoea included clinical identifications and treatment of dehydration seen in 131 (90.97%) who were given IV crystalloid solution, similar to the study done by Dekate et al on management of acute diarrhoea in Emergency room (ER)and appropriate use of antibiotics wherever indicated 19. In this study paediatric participants with dehydration as classified by WHO, were managed with IV crystalloids, and point of care ultrasound was used to assess and monitor fluid status of the patients, also patients who had features of infections from the dirrhoea with blood stains or complication related to severe diarrhoea, such as aspiration pneumonia for those who were severe ill and had complicated to aspiration pneumonia and most had elevated white blood cells from the full blood counts were managed with IV antibiotics, other were given IV antibiotics based on the clinical examinations findings.
Strength of the study
The main strength was a prospective cohort study with consecutive recruitment of participants. Hence participants had a good chance to follow up on data and record findings. A structured questionnaire was used to capture all the necessary information. Missing data was minimized as a large number of variables were captured.
Study limitation and mitigation
Some of the limitations expected while doing this study include accuracy in making a definition of acute diarrhea, but this was mitigated by using the Bristol stool chart to assess the consistency of the stool.
In this study, fewer patients were seen either as referral cases or self-referral due to the seasonal fluctuations of pediatric patients who presented with acute watery diarrhea during the study period
Conclusion
In this study we found that pediatric patients under 2 years of age were at high risks of severe diarrhea. Hypokalemia and referral from other facilities were the independent predictor of outcomes.
Recommendations
This study has revealed that severe diarrhea affects mostly pediatric patients with an age group below 2 years of age, and the predictors of outcomes were hypokalemia and referral status, which were statistically significant with p-value < 0.05, in the univariate and multivariate analysis, Thus, the following recommendations are hereby presented:
Further study should be done on the same topic in other places where emergency care is done to externally validate the finding of this study as it was single centered.
Earlier and immediate identification of under 5 children with diarrhea and appropriate interventions to prevent development of complications related to severe diarrhea.
Declarations
Ethics approval and consent to participate
The ethical approval was obtained from MUHAS IRB, with an ethical approval No. MUHAS-REC-02-2022-951, and permission from MNH research and consultancy bureau to use its patients and file notes. Consent was obtained from the patients before the start of the study and confidentiality was maintained during and after the study by safely keeping the study materials. De-identification at data entry was done to minimize direct association of patients’ details with the data. Only personnel directly involved with the research had access to the data. Information gathered should be used only for purposes of research and resultant publication.
From this study, there was no benefit to the patient, but the information obtained from the study will help in knowing where more efforts should be directed so as to improve the care that the paediatric patients presenting with severe diarrhoea receive in the EMD MNH, Tanzania.
We anticipated that no harm would come to those participants of the study as all the patients had received all the care as per the protocol of the EMD MNH where the study was conducted.
Consent to publish
Not applicable
Authors contributions
MJY was involved in the study design conceptualization, data collection, analysis and interpretation, drafted the manuscript, and made all necessary changes to the manuscript.
HRS, SSK and EW were involved in the study design conceptualization, review of the data analysis and interpretation, and critical review of the manuscript. CS, MAG and WM were involved in interpretation and revision of the manuscript. JM was involved in study design, data analysis and interpretation and review of manuscript.
Abbreviations
- EMD
- Emergency Medicine Department
- GAPPD
- Global Action Plan for Prevention and Control of Pneumonia and Diarrhoea
- IBM
- International Business Machines Corporation
- IMCI
- Integrated Management of Childhood Illnesses
- IRB
- Institutional Review Board
- LIC
- Low Income Country
- LMIC
- Low- and Middle-Income Country
- LTD
- Limited
- MNH
- Muhimbili National Hospital
- MUHAS
- Muhimbili University of Health and Allied Sciences
- ORS
- Oral Rehydration Salt
- PICU
- Paediatric Intensive Care Unit
- SPSS
- Statistical Package for the Social Sciences
- SSA
- Sub-Saharan Africa
- USA
- United States of America
- WHO
- World Health Organization
References
- 1.Imdad A, Mayo-Wilson E, Herzer K, Bhutta Z A. (2017) Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. Cochrane Database Syst Rev.
- 2.Brown K H, Peerson J M, Baker S K, Hess S Y.Preventive zinc supplementation among infants, preschoolers, and older prepubertal children. Food Nutr Bull. 2009-30.
- 3.Suehara Y, Yazawa Y, Hitachi K, Terakado A.Clear cell sarcoma arising from the chest wall: A case report. , J Orthop Sci 9(2), 171-4.
- 4.Bojalil R, Guiscafre H, Espinosa P, Viniegra L, Martõ H et al. (1999) Policy and Practice A clinical training unit for diarrhoea and acute respiratory infections an intervention for primary health care physicians in. , Mexico
- 5.Health A.WHO recommendations on the management of diarrhoea and pneumonia in HIV-infected infants and children. 2010.
- 6.Gebreyesus A, Id W, Dejene T A, Teferi M, Negash L et al.Risk factors for diarrhoea and malnutrition among children under the age of 5 years in the Tigray Region of Northern Ethiopia. 2018-32.
- 7.Ugboko H U, Nwinyi O C, Oranusi S U, Oyewale J O. (2020) Childhood diarrhoeal diseases in developing countries. Heliyon [Internet].
- 9.Paul E, Edwin P, Azage M.Geographical Variations and Factors Associated with Childhood Diarrhea in Tanzania A National Population Based Survey. 2015-16.
- 10.Whelan K, Judd P A, Preedy V R, Taylor M A, Pr P.Enteral feeding the effect on faecal output , the faecal microflora and SCFA concentrations. 2004-105.
- 11.Whelan K, Judd P A, Taylor M A.Defining and reporting diarrhoea during enteral tube feeding: Do health professionals agree?. , J Hum Nutr Diet 16(1), 21-6.
- 12.Daʇ G S, Dicle A, Saka O, Whelan K.Assessment of the Turkish version of the king’s stool chart for evaluating stool output and diarrhea among patients receiving Enteral nutrition. , Gastroenterol Nurs 38(3), 218-25.
- 13.Armon K, Stephenson T, MacFaul R, Hemingway P, Werneke U et al.An evidence and consensus based guideline for the management of a child after a seizure. , Emerg Med J 20(1), 13-20.
- 14.Nc O, Au C. (2015) Pattern of morbidity and mortality of childhood illnesses at the children emergency room of Abia State University Teaching Hospital . , Aba , Nigeria
- 15.Gorelick M H, Shaw K N, Murphy K O.Validity and reliability of clinical signs in the diagnosis of dehydration in children. , Pediatrics 99(5).
- 16.Ndikubwimana J B, NGENDAHIMANA F. (2020) Risk Factors Associated with Under-Five Diarrhea and Their Effect on Under-Five Mortality in Rwanda: Secondary Data Analysis of 2014-2015 Rwanda Demographic and Health Survey. SSRN Electron J.
- 17.DAG.Electrolyte Disturbances in Children Presenting with Acute Diarrhea: A Prospective Cohort Study. , J Med Sci Clin Res 7(09), 777-83.