
Efficacy and Safety of Lercanidipine Combination in Hypertensive Patients
Abstract
Calcium channel blockers (CCBs) are widely used for the treatment of arterial hypertension, but they differ in terms of pharmacology, tolerability, and pleiotropic actions. Lercanidipine, a highly lipophilic third generation dihydropyridine, reduces blood pressure (BP) effectively as monotherapy and in combination without inferiority to other major antihypertensive classes. We systematically searched PubMed and the Cochrane Library (last update: September 1, 2025) and screened reference lists for additional studies. Evidence from dose finding trials, randomized controlled studies, large observational cohorts, and meta analyses shows clinically meaningful reductions in office, home, and ambulatory BP with lercanidipine, including in patients with diabetes, obesity, chronic kidney disease, or high cardiovascular (CV) risk. Fixed- dose combinations with renin angiotensin system blockers (e.g., enalapril) provide greater BP reductions than monotherapy and are associated with favorable neurometabolic profiles. Beyond BP control, lercanidipine improves central hemodynamics and arterial stiffness, favors endothelial biology, and contributes to left ventricular hypertrophy regression. Across comparative trials, lercanidipine is generally better tolerated than older dihydropyridines. Presents lower rates of vasodilatory adverse events, less sympathetic activation, while discontinuations due to adverse events are uncommon. Overall, lercanidipine particularly within single pill combinations offers effective, durable BP lowering across diverse patient profiles with a favorable safety and tolerability profile and pleiotropic benefits that extend beyond BP reduction.
Figure 1. Graphical Abstract: Pleiotropic effects of Lercanidipine
Download figure
Article Information
- Received
- Accepted
- Published
Academic Editor: Sasho Stoleski, Institute of Occupational Health of R. Macedonia, WHO CC and Ga2len CC
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2025 Athanasios J Manolis, et al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Manolis S Kallistratos, Cardiology Department, Metropolitan Hospital, Piraeus, Greece —
Competing Interests
None
Funding
This work was supported by Berlin-Chemie AG, with its registered office at Glienicker Weg 125, 12489 Berlin, Germany.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Hypertension is the most common and probably the most important modifiable risk factor responsible for more than 10.000.000 deaths worldwide 1. It remains the leading cause of cardiovascular (CV) morbidity and mortality responsible for more than 50% of stroke, 45% of ischemic heart disease (IHD) and 25% of other CV diseases globally 2. Lifestyle modification and pharmacotherapy are the cornerstones for the management and treatment of arterial hypertension (HTN). Current ESH guidelines for the management of arterial hypertension recommend the use of lifestyle changes and/or (according to the total CV risk, and blood pressure (BP) levels) the use of the five major antihypertensive drug classes (Angiotensin- converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs), Calcium channel blockers (CCBs), diuretics and beta blockers (BB)) in order to decrease the hypertensive burden and control BP levels 4. While there are some differences for some cause-specific outcomes (less stroke prevention with BBs and ACE-inhibitors, less HF prevention with CCBs, and greater HF prevention with Thiazide diuretics), all major antihypertensive drugs effectively lower SBP and DBP, reduce the major specific outcomes associated with hypertension when compared with placebo; and exert an overall similar or only slightly different effect on the combined risk of major CV outcomes and mortality when given as the initial treatment step, highlighting the importance of tailored treatment based on individual patient characteristics. In the majority of hypertensive patients, when antihypertensive treatment is needed, current guidelines recommend the use of combination treatment (fix combinations if it’s feasible) in order to decrease and control BP levels 4. The recommendation of fix combinations occurred because they have superior BP reduction effects when compared with monotherapy, thus increasing the percentage of patients with controlled BP levels, decreasing, on the other hand, the physician’s inertia regarding arterial hypertension 4. Lercanidipine is a lipophilic third- generation calcium-channel blocker (CCB) with significant BP lowering as well as pleiotropic effects. In this article, we are going to review the published data regarding the efficacy of this drug in monotherapy or combination therapy, as well as the data regarding the tolerability, pleiotropic effects, and adverse events of Lercanidipine.
Materials and Methods
We conducted a focused literature search of PubMed/MEDLINE and the Cochrane Library from inception to September 1, 2025, using the terms lercanidipine, lercanidipine enalapril, calcium channel blocker and hypertension. Eligible studies included randomized controlled trials, prospective or retrospective observational studies, and meta-analyses evaluating lercanidipine as monotherapy or in combination in adult patients with hypertension. Primary outcomes were clinic, home and ambulatory blood pressure changes as well as tolerability,adverse events, secondary outcomes included central hemodynamics, renal parameters (albuminuria, proteinuria), metabolic effects and cardiovascular events. We excluded case reports, pediatric populations, non hypertensive indications, non peer reviewed sources, and non-English publications. Two authors independently screened titles, abstracts and reviewed full texts when needed, and extracted data. Discrepancies were resolved by consensus. Owing to heterogeneity in study designs and endpoints, findings were synthesized narratively without quantitative pooling.
Efficacy of Lercanidipine in randomized, observational studies and meta-analysis
Lercanidipine was first assessed in dose finding studies where single doses of 10 to 20 mg as well as 20 to 40 mg daily showed a significant BP-lowering effect in patients with mild to moderate 5, 6, 7, and severe HTN respectively 8. In the ELYPSE trial (Eficacia de Lercanidipino y su Perfil de Seguridad), a large non-comparative observational study that enrolled 9059 patients with mild to moderate HTN 9, 10 mg once daily administration of Lercanidipine decreased significant BP levels after 3 months of treatment (from 160.1 +/- 10.2/95.6 +/- 6.6 mmHg to 141.4 +/- 11.3/ 83.1 +/- 6.9 mmHg p < 0.001 versus baseline). In addition, a BP < 140/90 mmHg) was achieved in 32% of the patients. Moreover, in a large observational phase IV study that enrolled 2199 HTN patients, treatment with the over mentioned drug (10 to 20 mg as monotherapy, substitution of another drug because of adverse effects, or as add-on therapy) significantly decreased BP levels, with 63% of the patients reaching BP levels < 140/90 mmHg 10. Similar results were obtained in an open study that enrolled 756 hypertensive patients. The addition of lercanidipine (10 mg/day) as monotherapy effectively reduced BP levels after 8 weeks of follow up 11.
Lercanidipine combination
As expected, the combination of Lercanidipine with another antihypertensive drug led to a more marked decrease in BP levels when compared to monotherapy, regardless of the initial drug used (ACEi, ARB, a ß-blocker, or diuretic) 12, 13, 14, 15. In a randomized double-blind control study that enrolled 854 HTN patients, the combination of Lercanidipine with enalapril decreased home BP levels to a greater extent than the corresponding monotherapies and placebo (fall with monotherapies (-8.8/-5.9 mmHg, P < 0.001/<0.001 vs. placebo) with combination treatment (11.6/-7.6 mmHg, P < 0.001/< 0.001 vs. placebo and P < 0.01/< 0.05 vs. monotherapy) 14.
Lercanidipine enalapril fixed dose combination
Similar findings were observed with Fixed-Dose Single-Pill Combinations (SPC) containing lercanidipine 16, 17, 18. In a double-blind, placebo-controlled trial, 1039 HTN patients were randomized to receive placebo, monotherapy with Lercanidipine (LE) (10 or 20 mg daily), monotherapy with Enalapril (E) 10 or 20 mg daily, or LE/E combination at the following daily doses: LE10/E10, LE10/E 20, LE20/10 mg and LE20/E20. As expected, combination therapy was superior to placebo at all doses for both office and home BP 17. Likewise, in an open-label, prospective interventional study, the authors administered Lercanidipine (LE) 10 mg in treatment naïve patients with stage I hypertension and LE 10 mg/enalapril (E) 10 mg in hypertensive patients with stage II hypertension 18. After a period of 6 weeks, if patients didn’t reach BP levels<140/90 mmHg were up-titrated to LE 10 mg/E 10 mg or LE 10 mg/E 20 mg, respectively, for a further 6 weeks. After 12 weeks of treatment, BP levels decreased significantly by 16/7 mmHg for day time (systolic and diastolic BP levels respectively) (p<0.0001) and 13/7 mmHg for night time (P<0.009) in the ambulatory BP measurement 18. Lastly, in a meta-analysis that evaluated the efficacy and safety of lercanidipine/enalapril SPC in 9565 patients with mild to moderate essential hypertension, four observational studies treated with lercanidipine/enalapril SPC, were analyzed. Lercanidipine/enalapril SPC decreased SBP by 26 mmHg (95% CI, 23–29), and DBP by 13 mmHg (12–15), p < 0.05 16.
The use of fixed combinations with ace inhibitors and calcium channel blockers
Current ESH guidelines recommend the use of combination therapy in the majority of HTN patients since BP control with monotherapy is low 4. In addition, the use if SPC combinations decrease the number of pills to be taken, increasing thus patient’s adherence to treatment 4. Especially ACEi and CCB combination was extendedly assessed by many randomized controlled trials 19, 20, 21, 22, with significant results. The combination of these drugs decreases significantly BP levels and on the same time presents several significant pleiotropic effects that go beyond BP reduction 4, 19, 20, 21, 22. Moreover, the use of this combination decreases the rate of adverse events such as ankle edema while is metabolically neutral 4, 19, 20, 21, 22.
Comparison of Lercanidipine with Other Antihypertensive Drugs
Lercanidipine was compared in randomized controlled trials with all the major antihypertensive drug classes. In a double-blind controlled study, 217 patients with mild to moderate essential hypertension were divided in two groups receiving either lercanidipine 10 mg or atenolol 50 mg once daily 23. Βoth drugs showed similar BP-lowering efficacy. Similar results were observed when lercanidipine was compared with different angiotensin II receptor blockers (ARBs). In three different randomized controlled trials, Lercanidipine was compared against Losartan 24, 25, and Telmisartan 26. Once again, BP reduction was similar for both groups of drugs. Likewise, the comparison of lercanidipine with captopril 27, as well as with hydrochlorothiazide 28, 29, in three more randomized controlled studies showed that practically, the magnitude of BP reduction of lercanidipine in monotherapy is similar to that of the other major antihypertensive drug classes (Figure 2).
Figure 2. Percentage of normalized patients after treatment with the five major antihypertensive drug classes.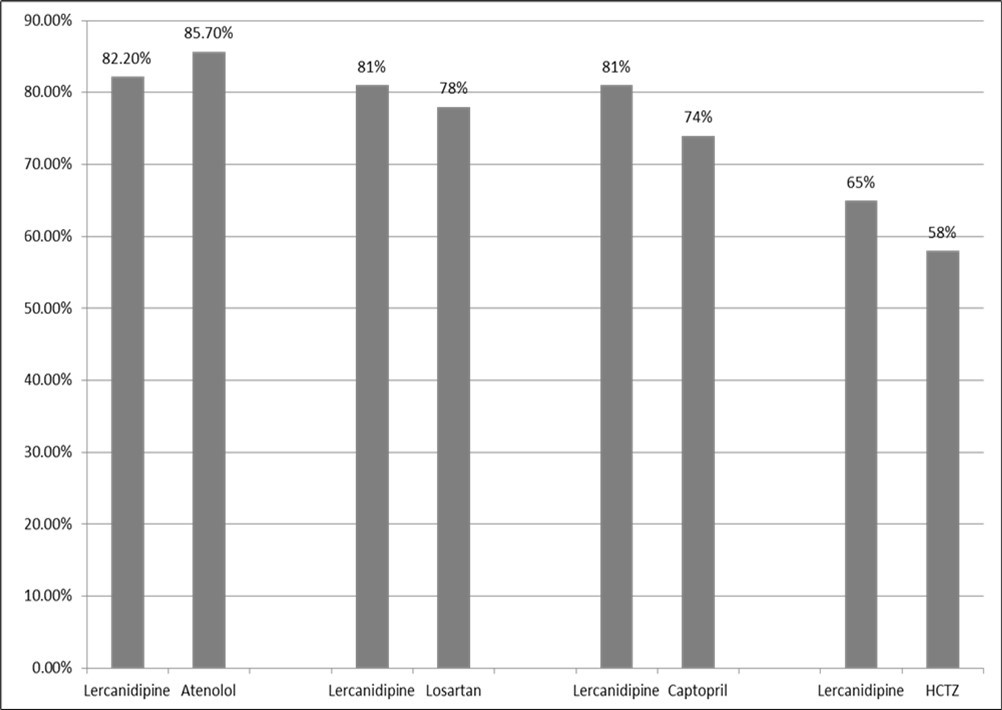
Download figure
Lercanidipine was also compared with other CCBs such as amlodipine, lacidipine, and nifedipine gastrointestinal therapeutic systems (GITS). In a multicenter, double-blind, parallel study, 828 HTN patients ≥60 years, were randomized to receive lercanidipine 10 mg/day, amlodipine 5 mg/day, or lacidipine 2 mg/day in a ratio 2:1:1 30. In this study, there were no significant differences in SBP and DBP reductions obtained by the three treatment regimens. Likewise, in another controlled study, 324 HTN patients were randomized to receive lercanidipine 5 mg, lacidipine 2 mg, or nifedipine 30 mg for 24 weeks. All three treatment regiments decreased similarly systolic blood pressure, while the decrease in diastolic blood pressure in the lercanidipine group (-18.3 mmHg) and in the nifedipine group (-17.7 mmHg) surpassed that in the lacidipine group (-16.6 mmHg) 31. Moreover, in the TOLERANCE study, the authors compared the effectiveness and tolerability of high doses of lercanidipine (20 mg) with amlodipine (10 mg) and nifedipine GITS (60 mg), in 650 patients with essential hypertension 32. Although the antihypertensive effect of all drugs was similar, signs and symptoms related to vasodilation were significantly higher (P < 0.001) in the amlodipine/nifedipine GITS group (76.8%, CI 95% 70.7; 82.9) than in lercanidipine group (60.8%, 56.1;65.5). Lastly, in a recent multicenter, retrospective observational study with 47,640 hypertensive patients, patients treated with amlodipine or lercanidipine were assessed. Both drugs demonstrated comparable effectiveness in terms of major adverse cardiac events prevention (2.8% vs. 4.1%, P = 0.11) 33.
The use of Lercanidipine in hypertensive patients with comorbidities
The majority of HTN patients usually present overlapping comorbidities and risk factors. Several studies have addressed this issue, assessing the therapeutic efficacy of lercanidipine in patients with insulin-independent diabetes, chronic kidney disease, obesity, and high-risk patients.
As expected, apart from the significant BP-lowering effect, lercanidipine in monotherapy or add-on therapy in patients with insulin-independent diabetes doesn’t affect glucose homeostasis parameters 34. Several randomized controlled studies affirm that combination treatment of a renin-angiotensin-system (RAS) blocker with lercanidipine is superior in terms of metabolic control when compared to diuretics 4. Moreover, the antihypertensive efficacy of lercanidipine is not affected by the body mass index or excess body fat. Several observational studies 35, 36, demonstrate the significant antihypertensive effect of this drug in this challenging population.
It’s well known that glomerular pressure regulation is impaired in patients with HTN. The vast majority of the CCBs vasodilate only afferent arterioles of the glomerulus affecting glomerular pressure and increasing the risk of time-dependent glomerular damage. According to studies in animal models, lercanidipine vasodilates both afferent and efferent arterioles, effect that may be beneficial in patients with hypertension and renal disease 37. Moreover, in the DIAL study (diabete, ipertensione, albuminuria, lercanidipina) 38, a multicenter, double-blind, active- controlled, parallel-group trial, 277 HTN patients were randomized to receive 10-20 mg/day of lercanidipine or 5-10 mg/day of ramipril and followed up for 9-12 months. In both groups, there was a significant reduction in albumin excretion rate (-17.4+/-65 microg/min for lercanidipine (p<0.05) and -19.7+/-52.5 for ramipril (p<0.05)). Likewise, there are several studies affirming that lercanidipine decreases proteinuria in patients with proteinuric renal disease 39, 40. Finally, in the RED LEVEL study, the authors compared the effects of lercanidipine + enalapril and amlodipine + enalapril combinations on renal parameters in HTN patients 41. In this study, apart from the BP reduction, albuminuria was significantly decreased with the lercanidipine + enalapril combination at 3, 6 and 12 months (changes from baseline were: -162.5 (p-value = 0.0439), -425.8 (p-value = 0.0010), -329.0 (p-value = 0.0011) mg/24 h), respectively). This effect was not observed with enalapril + amlodipine administration.
The efficacy of lercanidipine was also assessed in patients with high CV risk 42. In this study, the magnitude of BP reduction was related to CV risk levels. The higher the CV risk, the more pronounced the BP reduction.
Pleiotropic effects of Lercanidipine
Apart from the renoprotective effects mentioned above, several studies affirm that lercanidipine decreases not only peripheral BP but also central BP levels, aortic pulse pressure, and pulse wave velocity 43. When lercanidipine was compared with an ACEi (perindopril), a β- blocker (atenolol), or a diuretic (bendrofluazide) in a randomized study with elder patients with isolated systolic hypertension, all 4 classes of drugs reduced peripheral pulse pressure to the same extend however only perindopril, lercanidipine, and bendrofluazide significantly reduced central pulse pressure. In addition lercanidipine showed a more pronounced reduction of augmentation index 43. In addition, this drug exerts a significant vascular endothelial protective effect 44, since it increases the number of circulating endothelial progenitor cells ((CD34+/CD133+/VEGFR-2 + cells: 78.3 ± 64.5 vs 46.6 ± 32.8; CD34+/VEGFR-2+: 87996 ± 165116 vs 1026 ± 1559, respectively, p < 0.05, after 4 weeks of treatment). Moreover, in a pilot study, lercanidipine administration was associated with an improvement of peripheral, microcirculation, retinal circulation, and vasa vasorum networks 45. The presence of left ventricle hypertrophy (LVH) practically reflects the hypertensive burden of the patient and is associated with an increased risk of CV morbidity and mortality 4. Regression of LVH is translated into an improvement in CV prognosis since it reflects the decrease not only of the hypertensive burden but also reduces the harmful effects of LVH per se.3 Several randomized controlled studies have shown that lercanidipine decreases not only LVH, but also improves diastolic function 46, 47, 48.
Metabolic effects of lercanidipine/enalapril fixed combination
Several studies affirm that lercanidipine exerts a neutral or even favorable effect on lipid and glycemic profile 32, 35, 40, 49. Similar results were obtained when lercanidipine was combined with an angiotensin converting enzyme inhibitor (ACEi) or an angiotensin-II receptor blocker (ARBs) 12. In a prospective observational study that enrolled 162 patients with uncomplicated primary hypertension, combination of lercanidipine with an ACEi or ARB decreased significantly apart from BP levels, also fasting plasma glucose and serum levels of triglycerides 12. In addition, in a randomized, double-blind study that enrolled 120 hypertensive patients, L/E SPC decreased significantly lipoprotein(a) ((P < 0.001 vs. baseline) 50. Finally, in a randomized double-blind crossover study the authors compared L/E combination with enalapril–felodipine combination in order to assess the BP lowering effects of these drugs as well as the effects of the drugs in the neurometabolic alterations and homeostasis model assessment (HOMA) index in obese hypertensive patients 36. For the same ambulatory blood pressure monitoring (ABPM) BP levels reduction L/E combination decreased HOMA index while in the felodipine/enalapril group remained unchanged. Moreover, felodipine/enalapril group showed a more pronounced sympathetic activation in comparison to the LE group 36.
Safety, tolerability and adverse events of Lercanidipine
The majority of the dihydropyridine CCBs, activates sympathetic nervous system increasing heart rate and cardiac output, enhancing the risk for a subsequent arrhythmic event 51. On the other hand, lercanidipine seems to decrease sympathetic overdrive associated with hypertension. Chronic administration of lercanidipine doesn’t increase norepinephrine plasma concentration while decreasing muscle sympathetic nerve traffic 52. The most common adverse events (AE) induced by DHP-CCBs are related to systemic vasodilation and include ankle edema, dizziness, headache, flushing, palpitations, and vertigo. Lercanidipine may present AE, however, to a lesser extent. In the ELLE study 31, the incidence of AE was 19.4% in the lercanidipine group, 28.4% in the nifedipine group, and 27.1% in the lacidipine group. More precisely, edema was 2.8% in the LE group, 7.5% in the lacidipine group, and 10.1% in the nifedipine group (Figure 3). Similar AE was observed in another randomized controlled trial,29 where edema-related symptoms were significantly higher with amlodipine 50% than with LE 35% and lacidipine 34% (p<0.01). In a meta-analysis that included 8 RCTs (from 39 identified), the authors concluded that first generation CCBs presented higher risk than LE and second-generation, dihydropyridine CCBs of peripheral edema and a treatment withdrawal because of peripheral edema 53.
Figure 3. Incidence of adverse event and edema in different calcium channel blockers.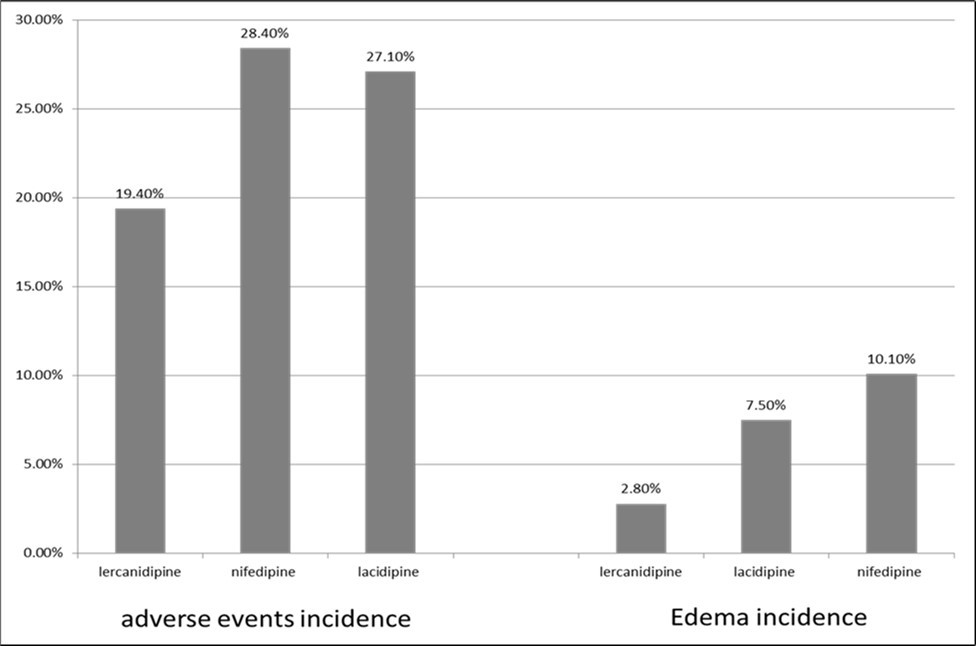
Download figure
Conclusions
Lercanidipine in monotherapy or combination therapy exerts a significant BP-lowering effect that is not inferior to the other major antihypertensive drug classes and is maintained after long-term treatment. The BP-lowering effect of this drug has been demonstrated in a wide range of patients with different comorbidities and risk factors, while at the same time presenting significant pleiotropic effects that go beyond BP reduction. Lastly, compared to the other DHP CCBs, it is better tolerated with a low rate of discontinuations due to AE, characterized by a low incidence of peripheral edema and a decrease in sympathetic activation.
References
- 1.GBD. (2019) Risk Factors Collaborators. “Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study. , Lancet 396(10258), 1223-1249.
- 2.Lawes C M. (2001) Vander Hoorn S, Rodgers A; International Society of Hypertension. “Global burden of blood-pressure-related disease. , Lancet 371(9623), 1513-8.
- 3.Whelton P K, Carey R M, Aronow W S, Casey DE Jr, Collins K J. (2017) ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. , Circulation 138(17), 10-1161.
- 4.Mancia G, Kreutz R, Brunström M, Burnier M, Grassi G. (2023) ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA). , J Hypertens 41(12), 1874.
- 5.Ambrosioni E, Circo A. (1997) Activity of Lercanidipine Administered in Single and Repeated Doses Once Daily as Monitored Over 24 Hours in Patients with Mild to Moderate Essential Hypertension”.Journal of Cardiovascular Pharmacology. 29-16.
- 6.Omboni S, Zanchetti A. (1998) Antihypertensive efficacy of lercanidipine at 2.5, 5 and 10 mg in mild to moderate essential hypertensives assessed by clinic and ambulatory blood pressure measurements. Multicenter Study Investigators”. Hypertens. 16(12), 1831-8.
- 7.Circo A. (1997) Active Dose Findings for Lercanidipine in a Double-Blind, Placebo-Controlled Design in Patients with Mild to Moderate Hypertension”.Journal of Cardiovascular Pharmacology. 29-21.
- 8.Paterna S, Licata A, Arnone S, Cottone C, Corrao S et al. (1997) Lercanidipine in Two Different Dosage Regimens as a Sole Treatment for Severe Essential Hypertension”.Journal of Cardiovascular Pharmacology. 29-50.
- 9.Barrios V, Navarro A, Esteras A, Luque M, Romero J. (2002) Antihypertensive efficacy and tolerability of lercanidipine in daily clinical practice. The ELYPSE Study. Eficacia de Lercanidipino y su Perfil de Seguridad”. Blood Press. 11(2), 95-100.
- 10.Burnier M, Gasser U E. (2007) Efficacy and tolerability of lercanidipine in patients with hypertension: results of a Phase IV study in general practice. Expert Opin Pharmacother. 8(14), 2215-23.
- 11.Poncelet P, Ribstein J, Goullard L. (2004) la tolérance de la lercanidipine ne sont pas liées à l'âge des patients hypertendus: étude AGATE [Efficacy and acceptability of lercanidipine are not age dependent in patients with essential hypertension: the AGATE study].Ann Cardiol Angeiol(Paris). 53, 123-30.
- 12.Cicero A F, Gerocarni B, Rosticci M, Borghi C. (2012) Blood pressure and metabolic effect of a combination of lercanidipine with different antihypertensive drugs in clinical practice”. Clin Exp Hypertens. 34(2), 113-7.
- 13.Guillen Gil, Abellan Jose, Jose Luis Llisterri. (2003) P-212: Efficacy and safety of lercanidipine in combination with enalapril in HBP. Preliminary results of Zanycontrol study group”.American Journal of Hypertension. 16-1.
- 14.Mancia G, Omboni S, Chazova I, Coca A, Girerd X. (2016) Effects of the lercanidipine-enalapril combination vs. the corresponding monotherapies on home blood pressure in hypertension: evidence from a large database”. J Hypertens. 34(1), 139-48.
- 15.Yang Z. (2015) Efficacy and safety evaluation of perindopril-lercanidipine combined therapy in patients with mild essential hypertension”. Curr Med Res Opin. 31(1), 183-6.
- 16.Rizzoni D. (2016) Fixed-dose lercanidipine and enalapril in field practice: a meta-analysis”. Curr Med Res Opin. 32, 13-15.
- 17.Mancia G, Coca A, Chazova I, Girerd X, Haller H al. (2014) Effects on office and home blood pressure of the lercanidipine-enalapril combination in patients with Stage 2 hypertension: a European randomized, controlled clinical trial”. J Hypertens. 32(8), 1700-7.
- 18.Rayner B. (2019) The effect of lercanidipine or lercanidipine/enalapril combination on blood pressure in treatment-naïve patients with stage 1 or 2 systolic hypertension”.Pragmatic and Observational Research. 10, 9-14.
- 19.Wang J G, Staessen J A, Gong L, Liu L. (2000) Chinese trial on isolated systolic hypertension in the elderly. Systolic Hypertension in China (Syst-China) Collaborative Group. Arch Intern Med. 160(2), 211-20.
- 20.Staessen J A, Fagard R, Thijs L, Celis H, Arabidze G G. (1997) Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet. 350(9080), 757-64.
- 21.Dahlöf B, Sever P S, Poulter N R, Wedel H, Beevers D G. (2005) Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet. 366(9489), 895-906.
- 22.Jamerson K, Weber M A, Bakris G L, Dahlöf B, Pitt B. (2008) ACCOMPLISH Trial Investigators. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. , N Engl 359(23), 2417-28.
- 23.Morisco C, Trimarco B.Efficacy and Tolerability of Lercanidipine in Comparison to and in Combination with Atenolol in Patients with Mild to Moderate Hypertension in a Double-Blind Controlled Study. Journal of Cardiovascular Pharmacology. 29:p S26-S30
- 24.James I G, Jones A, Davies P. (2002) A randomised, double-blind, double-dummy comparison of the efficacy and tolerability of lercanidipine tablets and losartan tablets in patients with mild to moderate essential hypertension”. J Hum Hypertens. 16(8), 605-10.
- 25.Lin T H, Voon W C, Yen H W, Huang C H, Su H M. (2006) Lercanidipine and losartan effects on blood pressure and fibrinolytic parameters”. Kaohsiung J Med Sci. 22(4), 177-83.
- 26.Sarafidis P A, Lasaridis A N, Hatzistavri L, Zebekakis P, Tziolas I. (2004) P-508: The effects of telmisartan and lercanidipine on blood pressure and insulin resistance in hypertensive patients”. , American Journal of Hypertension 17-1.
- 27.Barbagallo G Sangiorgi, Putignano E, Calcara L, Barbagallo M. (1997) Efficacy and Tolerability of Lercanidipine vs. Captopril in Patients with Mild to Moderate Hypertension in a Double-Blind Controlled Study”. Journal of Cardiovascular Pharmacology. 29-2.
- 28.Notarbartolo A, Rengo F, Scafidi V, Acanfora D. (1999) Long-term effects of lercanidipine on the lipoprotein and apolipoprotein profile of patients with mild-to-moderate essential hypertension”. Current Therapeutic Research, Clinical and Experimental;. 60, 228-236.
- 29.Burnier M, Pruijm M, Wuerzner G. (2009) Treatment of essential hypertension with calcium channel blockers: what is the place of lercanidipine?” Expert Opin Drug Metab Toxicol. 5(8), 981-7.
- 30.Leonetti G, Magnani B, Pessina A C, Rappelli A, Trimarco B et al. (2002) A; COHORT Study Group. Tolerability of long-term treatment with lercanidipine versus amlodipine and lacidipine in elderly hypertensives. J Hypertens. 15(11), 932-40.
- 31.Cherubini A, Fabris F, Ferrari E, Cucinotta D, Antonelli Incalzi R et al. (2003) Comparative effects of lercanidipine, lacidipine, and nifedipine gastrointestinal therapeutic system on blood pressure and heart rate in elderly hypertensive patients: the ELderly and LErcanidipine (ELLE) study. Arch Gerontol Geriatr. 37(3), 203-12.
- 32.Barrios V, Escobar C, M de la Figuera, Llisterri J L, Honorato J. (2008) Tolerability of high doses of lercanidipine versus high doses of other dihydropyridines in daily clinical practice: the TOLERANCE Study. Cardiovasc Ther. 26(1), 2-9.
- 33.Jeon J, Ryoo S, Oh S, Hong S J, Yu C W et al. (2025) . Comparative Effectiveness of Lercanidipine and Amlodipine on Major Adverse Cardiovascular Events in Hypertensive Patients. Am 38(2), 139-147.
- 34.Cleophas T J, van Ouwerkerk BM, Meulen J van der, Zwinderman A H. (2001) Diabetics with hypertension not controlled with ACE inhibitors: alternate therapies”. Angiology. 52(7), 469-75.
- 35.Barrios V, Calderon A, Navarro A, Noya C, Herranz I et al. (2004) Lercanidipine effectiveness and tolerability profile is not influenced by overweight or body fat increase. The LERZAMIG study. J Hypertens. 22-258.
- 36.Seravalle G, Brambilla G, Pizzalla D P, Casati A, Riva M. (2016) Differential effects of enalapril- felodipine versus enalapril-lercanidipine combination drug treatment on sympathetic nerve traffic and metabolic profile in obesity-related hypertension. J Am Soc Hypertens. 10(3), 244-51.
- 37.Sabbatini M, Leonardi A, Testa R, Vitaioli L, Amenta F.Effect of calcium antagonists on glomerular arterioles in spontaneously hypertensive rats. , Hypertension 35(3), 775-9.
- 38.Dalla Vestra M, Pozza G, Mosca A, Grazioli V, Lapolla A.Effect of lercanidipine compared with ramipril on albumin excretion rate in hypertensive Type 2 diabetic patients with microalbuminuria: DIAL study (diabete, ipertensione, albuminuria, lercanidipina). Diabetes Nutr Metab. 17(5), 259-66.
- 39.Robles N R, Pastor L, Manjón M, Ocón J, Campderá Gómez.Lercanidipine in diabetic patients with renal failure. , Nefrologia 24(4), 338-43.
- 40.Robles N R, Romero B, de Vinuesa EG, Sánchez-Casado E, Cubero J J. (2010) Treatment of proteinuria with lercanidipine associated with renin-angiotensin axis-blocking drugs. Ren Fail. 10-3109.
- 41.Robles N R, Calvo C, Sobrino J, Espinel E, Esteban R.. RED LEVEL trial (REnal Disease: LErcanidipine Valuable Effect on urinary albumin Loses) Curr Med Res Opin. 2016 Oct;32(sup2): 29-34.
- 42.Barrios V, Escobar C, Navarro A, Barrios L, Navarro-Cid J et al.Lercanidipine is an effective and well tolerated antihypertensive drug regardless the cardiovascular risk profile: The LAURA study”. , Int J Clin Pract 60(11), 1364-70.
- 43.Mackenzie I S, McEniery C M, Dhakam Z, Brown M J, Cockcroft J R et al.Comparison of the effects of antihypertensive agents on central blood pressure and arterial stiffness in isolated systolic hypertension”. , Hypertension 54(2), 409-13.
- 44.C De, Rossini C, Tincani A, Airò P, Scarsi M. (2016) Effect of antihypertensive treatment with lercanidipine on endothelial progenitor cells and inflammation in patients with mild to moderate essential hypertension. Blood Press. 25(6), 337-343.
- 45.Cesarone M R, Incandela L, Ledda A, De Sanctis MT, Steigerwalt R. (2000) Pressure and microcirculatory effects of treatment with lercanidipine in hypertensive patients and in vascular patients with hypertension. Angiology. 51-8.
- 46.Cuspidi C, Sala C, Negri F, Mancia G, Morganti A. (2012) Prevalence of left-ventricular hypertrophy in hypertension: an updated review of echocardiographic studies”. J Hum Hypertens. 26(6), 343-9.
- 47.Grandi A M, Solbiati F, Laurita E, Maresca A M, Nicolini E. (2008) Effects of dual blockade of Renin-Angiotensin system on concentric left ventricular hypertrophy in essential hypertension: a randomized, controlled pilot study”. , Am 21(2), 231-7.
- 48.Ter-Stepanyants E, Ordyan A, Aleksanyan L, Naghdalyan A. (2011) Effect of combined therapy with lercanidipine and ramipril on left ventricular hyperthrophy in elderly patients with isolated systolic hypertension”. , Journal of Hypertension. e563
- 49.Viviani G L. (2002) Lercanidipine in type II diabetic patients with mild to moderate arterial hypertension. , J Cardiovasc Pharmacol 40(1), 133-9.
- 50.Derosa G, Bonaventura A, Romano D, Bianchi L, Fogari E. (2014) Effects of enalapril/ lercanidipine combination on some emerging biomarkers in cardiovascular risk stratification in hypertensive patients. , J Clin Pharm Ther 39(3), 277-85.
- 51.Manolis A J, Poulimenos L E, Kallistratos M S, Gavras I, Gavras H. (2014) Sympathetic overactivity in hypertension and cardiovascular disease. Curr Vasc Pharmacol. 12(1), 4-15.