
Abstract
Background and Purpose
The ability to respond effectively to perturbations is a key element of reactive postural control and is a crucial mediator of falls. Several studies exist in the literature that determine older adults’ responses to perturbations, however those studies typically involve procedures that lack objectivity or applicability outside a laboratory. A study involving waist-pull perturbations with a spring-scale (SS) is an exception. In that study, fall history was most accurately differentiated by a reactive stepping response to a perturbing force of 10% total body weight. Using data from that study, we retrospectively examined the association between fall history and the number of steps accompanying a SS perturbing force of 10% total body weight in older adults. For perspective, the association of fall history with Timed-Up-and-Go (TUG) and single limb stance (SLS) times was also determined.
Methods
Fifty-eight healthy older adults (mean age = 80.7 years) participated in the study. Their 2-year fall history (yes, no) was recorded. All participants underwent SS testing with one-pound incremental, horizontal sagittal plane manual waist-pull perturbations. The number of steps in response to perturbation with 10% total body weight was recorded; TUG and SLS tests were performed. Associations between variables were examined using Spearman (rank-biserial) correlations.
Results
The median number of steps for fallers was 5 in both anterior and posterior directions. For non-fallers, the median number of steps was 1 and 2 in the anterior and posterior directions, respectively. The significant correlations between fall status and number of steps were 0.772 and 0.813 for the anterior and posterior directions, respectively. Similarly, the significant correlations between fall status and balance tests were 0.722 and -0.456 for the TUG and the SLS, respectively.
Conclusions
The number of steps accompanying waist-pull perturbations with forces of 10% of body weight were highly explanatory of experiencing a fall during the preceding 2 years.
Author Contributions
Academic Editor: Ian James Martins, Edith Cowan University, Australia.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Rachana Gangwani, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
Falls are a common occurrence among older adults that can result in injury, hospitalization, decreased mobility, fear of another fall, decreased quality of life, and even death. 1, 2, 3, 4, 5 Considering the higher fall incidence in older adults and its consequences, it is crucial to study factors that predispose older adults to falls and determine measures that can best identify those at fall-risk. Limited balance is one of the chief risk factors for falls. 6, 7, 8 Horak et al have proposed that 6 systems underlie balance, with “postural responses” to perturbations being one among them. 9 They incorporated postural reactions to perturbations in their Balance Evaluation Systems Test (BESTest)9 as did Rose et al in their Fullerton Advanced Balance (FAB) scale. 10 In both test batteries, the tester observes the tested individual’s response to the release of a push force. The postural responses are graded ordinally and take compensatory stepping into account.
Considering the subjective nature of grading postural responses, procedures for obtaining more objective measures of postural responses to perturbations have been described. 11, 12, 13, 14 However, they have involved the use of motorized treadmills or waist pulls and are not easily adopted for use outside a laboratory setting. An exception is the Repeated Incremental Predictable Perturbations Reactive Stepping (RIPPS) test which incorporates a portable spring scale (SS) tethered to the waist. 15 The test was described by DePasquale and Toscano over 10 years ago. They reported the maximum perturbation force (as a percentage of body weight) associated with an effective protective stepping response (limit 3 steps) had high test-retest reliability and was an excellent explanator of fall history. They found a force cut point of 10% of the total body weight as the most sensitive and specific explanator. They also found that the 10% total body weight criterion to be superior to Timed-Up-and-Go (TUG) and single limb stance (SLS) times as an explanator of fall history.
The purpose of the present study was to expand on the findings of the DePasquale and Toscano study. Specifically, we sought to determine the association between a history of falls and the number of steps accompanying a SS perturbing force of 10% total body weight in a sample of older adults. We hypothesized that the number of steps in response to 10% total body weight waist-pull unloading force would be associated with fall history. This hypothesis was based on evidence from the previous literature which indicated that individuals who resort to multiple stepping responses are at a higher risk of falls compared to those who take fewer or a single compensatory step to recover from a perturbation. 5, 11, 12 However, most of these studies resorted to perturbations induced via motorized treadmills and lean-release systems and indicated the need for specific tests that target the capacity to perform reactive stepping to identify those at risk of falls. 11, 12, 14, 16 Thus, if the hypothesis is proven, it will provide an opportunity to healthcare professionals to assess reactive stepping responses and differentiate fallers from non-fallers in clinical settings. For perspective, the association of fall history with TUG and SLS times was also determined. The present study is based on the secondary analysis of the data collected for the publication of the first study by DePasquale and Tascano in 2009. 15 As the previous study only assessed the reliability and validity of the SST and determined that 10% TBW measure can discriminate fallers from non-fallers and with a growing interest in the field of reactive balance assessment and the lack of simple, portable, feasible and objective tools for reactive balance assessment in clinical settings, we went back to the data collected from the SST to determine whether the reactive stepping response measures derived from the SST can correlate with fall history in older adults and thereby bridge the gap in the literature and provide healthcare professionals with a tool that assesses reactive stepping responses and identify those at risk of falls in clinical settings.
Methods
This retrospective study involved the secondary analysis of data from a study of the SS test. That study was approved by the Institutional Review Board.
Participants
Participants were recruited by personal request, flyers, or presentations (public or private). They were enrolled between January 2006 and 2007. The inclusion criteria for the participants were: 1) provision of informed consent, 2) ability to ambulate in the community unrestricted with or without a cane for one or more blocks, 3) age of 65 years or older, 4) ability to complete the TUG test in less than 14 seconds, 5) demonstration of medically stability without the need for medical adjustments or medical intervention, 6) absence of lower extremity pain, 7) absence of hospitalization, spinal or lower extremity fracture within 3 months of participation, 8) ability to stand unsupported without an assistive device, 9) weight of 200lbs or less, and 10) ability to understand and follow simple instructions in English. The exclusion criteria for participants were: 1) active dorsiflexion/plantarflexion range of motion of less than 10°, and 2) less than 3+/5 manual muscle test scores for ankle dorsiflexion and plantarflexion. A convenience sample of 61 participants was recruited. Following screening, 58 participants provided written informed consent and were enrolled in the study.
Procedures
Although focused on the RIPPS test, this study also involved the gathering of information relative to demographics and fall history. Additionally, two other balance tests were conducted. Demographics included gender, age, height, and weight. Fall history was ascertained by asking participants if they had fallen at least once in the past 2 years. A fall event was defined as a loss of balance during routine activities that resulted in their “trunk, knee, or hand unintentionally coming to rest on the ground, wall, table, chair or other surface.” 17 Fall exclusions included overwhelming environmental hazards (eg. violence, slipping on ice) or acute medical conditions (eg. collapse due to syncope). The other 2 balance tests performed were the TUG and SLS tests. For the TUG, participants stood from an armchair, walked past a mark on the floor 3.0 meters distant, turned, walked back to the chair, turned, and sat down. They were instructed to walk at a quick but safe speed. They were timed with a digital stopwatch from the command go until they returned to sitting. The SLS was timed from when participants began independent standing on their preferred lower limb until the contralateral lifted foot touched the floor, the stance foot moved, or 30 seconds was reached.
The RIPPS testing involved a pocket-sized SS (Pelouze/Pelstar LLC, Bridgeview, IL) with a 26lb (12 kg) capacity. The scale is capable of quantifying manual waist-pull forces in one-pound increments with a 0 set point turn dial calibration capacity. Further calibration accuracy of the linear SS was achieved through suspension of a 5-pound weight from the scale before the start of the test. The SS was attached to a 5-inch-wide belt that was secured around the participant’s waist. The SS was attached to the padded belt on one end and held on the other end by the examiner. A 4-foot tether strap was secured at waist level to both the examiner and the participant for safety (Figure 1).
Figure 1.SST Anterior direction waist pull testing (rear stepping) set up with one end of the spring scale attached to the participant’s waist and the other end held by the examiner. A tether strap is secured via a belt at waist-level to both the participant and the examiner for participant safe. The figure also depicts a clear view of the participant’s feet and the presence of compliant surface to ensure participant safety.
The RIPPS testing took place with participants standing on a firm unpadded surface in their normal footwear. Waist-pull perturbations were applied by the tester in the sagittal plane with the SS held parallel to the ground. The SS assessed the waist-pull perturbation force against which a person could maintain postural stability during both anterior and posterior direction perturbations. Before performing the RIPPS testing, participants practiced responding to continuous SS loading waist- pull forces to the maximum limits of foot-flat accommodation to familiarize them with the device and testing process. However, participants did not have a practice trial for “unloading.” Prior to and during RIPPS testing, examiners instructed participants to maximally resist waist-pull loading forces while maintaining foot-flat (heel-forefoot) floor contact and to use the fewest steps possible, in response to the sudden unloading/release of the loading waist-pull forces. Participants were informed that waist-pull loading forces would suddenly be unloaded without warning at the discretion of the examiner at each additional one-pound incremental force.
After the practice trial, RIPPS testing began with rounds of anterior direction loading and unloading of SS waist-pull forces to provoke posterior stepping. These were followed by posterior direction loading and unloading of SS waist-pull forces to provoke anterior stepping. For both directions loading began with a one-pound force. Each successive round increases the waist-pull force by one pound. During each round, the loading forces were gently administered to allow the participant time to accommodate. Successful foot-flat loading phase was followed by sudden, quasi-random unloading administered at the discretion of the examiner within a subjective 5 second window. Each successive round of increasing loading and unloading force continued to the maximal limits (see below) or until the subject failed either the loading or unloading SS performance criteria.
Measurements of force and stepping were obtained using the RIPPS procedure (Appendix A). Threshold force was the minimum waist-pull force (as a percentage of total body weight) at which a participant demonstrated the initial onset of a stepping response during unloading. Threshold stepping represented the number of steps required by the participant to regain balance in response to a threshold unloading force. Limit force was the maximum waist-pull force (as a percentage of total body weight) at which an effective protective stepping response (3 step criterion) could be sustained irrespective of the whether it occurred with loading or unloading. The third measurement was the number of steps taken to regain balance on unloading of a waist-pull perturbation of 10% total body weight. This was the primary explanatory variable of interest in this study.
Appendix A. RIPPS SST PROTOCOL| Component | Method | Purpose | End Point Performance Criteria |
| AnteriorFacing subjectLoading | Continuous 1 lb incremental loading forces applied in a gentle / accommodative fashion | Assess non - stepping effective accommodation foot flat limits. | No stepping to x% total body weight or %TBW where loss of foot flat contact or stepping response occurs. |
| anterior Facing subjectLoading/unloading | Cyclic 1 lb incremental loading/unloading | To assess effective back stepping limits expressed as percent of total body weight. % TBW | >3 steps observed or contact with support surface. % TBW at highest successful trial observed. |
| IposteriorSubject’s back to examinerLoading | Continuous 1 lb incremental loading forces applied in a gentle/accommodativefashion | Assess non - stepping effective accommodation foot-flat limits | No stepping to x% TBW at point of stepping or loss of foot flat contact. |
| PosteriorSubject’s back to examinerLoading/unloading | Cyclic 1 lb incremental loading /unloading | To assess effective forward stepping limits expressed as percent of total body weight. % TBW | > 3 steps or support surface contact % TBW at highest successful trial observed. |
Data Analysis
All analysis was conducted with SPSS version 20.0 (IBM, Armonk, NY, USA) and MedCalc version 19.1.6 (MedCalc Software Limited, Ostend, Belgium) statistical packages. Basic descriptive statistics were calculated. Spearman (rank-biserial) correlations were used to examine the relationship between explanatory variables (steps at 10% body weight, TUG times, and SLS times) and fall history (yes = 1, no = 0).
Results
Of the 58 participants, 19 were men and 39 were women. The mean (SD) and range of their ages were 80.7(7.2), 65-94 years, of their height were 165.3(10.2), 135.0-185.0 cm, and of their weight were 67.8(12.4), 46.7-90.2kg. Twenty-nine reported having fallen in the past 2 years. Table 1 summarizes explanatory variables relative to fall history.
Table 1. Summary of Explanatory Variables and Their Relationship with Fall History*| Explanatory Variables | Fallers(n=29) | Non-fallers(n=29) | Correlationᵻ | 95% CI |
| Anterior steps at 10% weight (n) | 5 (1-5) | 1 (0-5) | 0.772 | 0.641 - 0.859 |
| Posterior steps at 10% weight (n) | 5 (1-5) | 2 (1-5) | 0.813 | 0.703 - 0.886 |
| Timed Up & Go (s) | 9.2 (1.3) | 7.0 (1.0) | 0.722 | 0.569 - 0.826 |
| Single limb stance time (s) | 3.2 (3.3) | 10.3 (9.6) | -0.454 | -0.637 - 0.221 |
(Figure 2a and Figure 2b) indicate the number of anterior and posterior steps taken by fallers and non-fallers in response to unloading 10% total body weight waist-pull force. These data are further summarized in Table 1 as is participant performance on the TUG and SLS tests and the relationship between all explanators and fall history. All balance tests provided a significant (p<.001) explanation of fall history. The correlations of number of steps and TUG times with fall history (rs = 0.722 to 0.813) were all positive and were not significantly different in magnitude. Thus, indicating that participants who took more steps in response to the unloading 10% total body weight waist-pull perturbation force or required more time to complete the TUG were more likely to have fallen. The correlation between SLS times and fall history was negative- suggesting that participants who could not balance as long on one lower limb were more likely to fall. This correlation was also of significantly less magnitude and therefore a weaker explanator of fall status than the other balance variables.
Figure 2a.Bar graph illustrating number of anterior steps taken in response to a 10% perturbation force by individuals with a history of falls (no vs yes).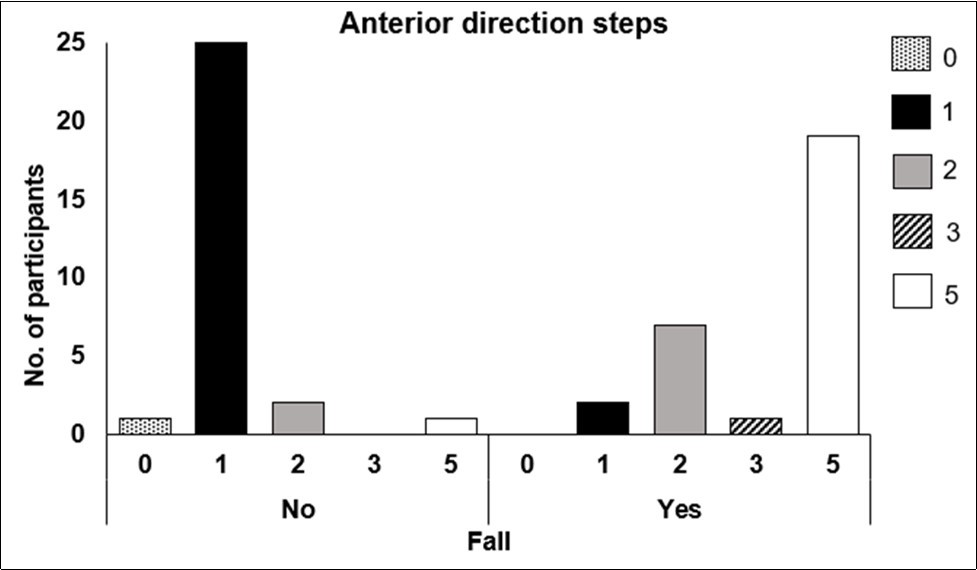
Figure 2b.Bar graph illustrating number of posterior steps taken in response to a 10% perturbation force by individuals with a history of falls (no vs yes).
Discussion
When perturbations of sufficient magnitude are encountered, appropriate postural responses are required if a fall is to be avoided. 9 Considerable research has focused on quantifying postural responses to motor (treadmill or waist-pull) generated perturbations. 11, 12, 13, 14 While informative, the research does not translate well to clinical practice. An alternative, the RIPPS system, is portable and has already been shown in community settings to differentiate between older adults with and without a history of falling on the basis of their response to a perturbation force equal to 10% of total body weight. The purpose of this study was to further examine the ability of the RIPPS system to differentiate between individuals with and without a fall history, but on the basis of the number of steps they took in response to a constant perturbation force (10% total body weight) applied at the waist via a spring scale.
The study clearly showed that the number of steps taken in response to unloading 10% perturbation force, whether anterior or posterior, was higher among fallers than non-fallers. Our study indicated that the median number of steps for fallers was 5 in both anterior and posterior directions whereas non-fallers almost always took 2 or fewer steps, a number which is also referred to by Rose et al in the scoring of reactive postural control. 10 Previous literature has also demonstrated that a multiple stepping response to perturbations is common in fallers. 18, 19 This might be due to several reasons such as age-related changes in older adults and the inability to accurately assess the perturbation parameters, resulting in an ineffective first compensatory step and thus having to resort to multiple stepping strategy to regain balance. 16, 20 Thus, our study results support the literature that the ability to take an efficient single step response might be associated with a lower fall-risk, 5 thereby suggesting that examining the stepping strategy could be an essential component of fall-risk assessment.
The relationships between step number and fall history were strong and comparable to the relationship between TUG times and fall history. This is noteworthy as the TUG addresses different systems of balance, that is, “anticipatory postural adjustments” and “stability in gait”, 9 and is according to Lusardi et al, one of “the most evidence-supported functional measures to determine individual risk of future falls.” 21 The relationship between SLS, an example of an “anticipatory postural adjustment,” 9 and fall history was significant but only fair in magnitude.
This study has several limitations. First, it focused on only one measurement from the RIPPS. This was deemed appropriate as it incorporated a 10% perturbation force already shown to be explanatory.15 Second, the study used fall history as an indicator of fall status. The ability to predict future falls is of greater importance. Finally, the analysis of the present study while appropriate, was different from that of the earlier study using RIPPS data.15 This difference, while driven by characteristics of the step data, limits between study comparisons.
Conclusion
The number of steps taken in response to a 10% total body weight waist-pull perturbation is strongly related to fall history. However, future studies should validate and determine whether the step frequency at 10%TBW can predict real-life prospective falls, thereby further ensuring the use of SST in fall-risk assessment protocols.
Acknowledgements
None.
References
- 1.A J Campbell. (1990) Circumstances and consequences of falls experienced by a community population 70 years and over during a prospective study. , Age Ageing 19(2), 136-41.
- 2.A J Milat. (2011) Prevalence, circumstances and consequences of falls among community-dwelling older people: results of the 2009 NSW Falls Prevention Baseline Survey. , N S W Public Health Bull.22(3-4): 43-8.
- 3.B J Vellas. (1997) Fear of falling and restriction of mobility in elderly fallers. Age Ageing. 26(3), 189-93.
- 4.Stenhagen M. (2014) Accidental falls, health-related quality of life and life satisfaction: a prospective study of the general elderly population. Arch Gerontol Geriatr. 58(1), 95-100.
- 5.B E Maki, W E Mcilroy. (1999) Control of compensatory stepping reactions: age-related impairment and the potential for remedial intervention. Physiotherapy theory and practice. 15(2), 69-90.
- 6.D A Ganz, N K Latham. (2020) Prevention of Falls in Community-Dwelling Older Adults. , N Engl J Med 382(8), 734-743.
- 7.P E Magnani. (2019) Use of the BESTest and the Mini-BESTest for Fall Risk Prediction. in Community-Dwelling Older Adults Between 60 and 102 Years of Age. J Geriatr Phys Ther .
- 8.L T Southerland. (2017) Are triage questions sufficient to assign fall risk precautions in the ED? Am J Emerg Med. 35(2), 329-332.
- 9.F B Horak, D M Wrisley, Frank J. (2009) The Balance Evaluation Systems Test (BESTest) to differentiate balance deficits. Phys Ther. 89(5), 484-98.
- 10.D J Rose, Lucchese N, L D Wiersma. (2006) Development of a multidimensional balance scale for use with functionally independent older adults. Arch Phys Med Rehabil. 87(11), 1478-85.
- 11.J R Crenshaw, M D Grabiner. (2014) The influence of age on the thresholds of compensatory stepping and dynamic stability maintenance. Gait Posture. 40(3), 363-8.
- 12.B W Schulz, J A Ashton-Miller, N B Alexander. (2006) Can initial and additional compensatory steps be predicted in young, older, and balance-impaired older females in response to anterior and posterior waist pulls while standing?. , J Biomech 39(8), 1444-53.
- 13.D L Sturnieks. (2012) Sensorimotor and neuropsychological correlates of force perturbations that induce stepping in older adults. Gait Posture. 36(3), 356-60.
- 14.M L. (2003) Thresholds for inducing protective stepping responses to external perturbations of human standing. , J Neurophysiol 90(2), 666-74.
- 15.DePasquale L, Toscano L. (2009) The Spring Scale Test: a reliable and valid tool for explaining fall history. J Geriatr Phys Ther. 32(4), 159-67.
- 16.Joshi M, Patel P, Bhatt T. (2018) Reactive balance to unanticipated trip-like perturbations: a treadmill-based study examining effect of aging and stroke on fall risk. International Biomechanics. 5(1), 75-87.
- 17.L K Boulgarides. (2003) Use of clinical and impairment-based tests to predict falls by community-dwelling older adults. Phys Ther. 83(4), 328-39.
- 18.S E Lord, Weatherall M, Rochester L. (2010) Community ambulation in older adults: which internal characteristics are important? Arch Phys Med Rehabil. 91(3), 378-83.
- 19.Pijnappels M. (2010) The association between choice stepping reaction time and falls in older adults--a path analysis model. Age Ageing. 39(1), 99-104.